






Best Rotator Cuff Treatment in Mohali & Chandigarh | Fortis Mohali
By Dr Manit Arora Senior Consultant, Orthopaedics & Sports Medicine | Fortis Hospital, Mohali Australian-trained Orthopaedic & Sports Medicine Surgeon Fellowships: Shoulder & Knee Arthroscopy (Australia, France, Japan, USA) Visiting Faculty: AIIMS Rishikesh | IIM Rohtak | 15+ years, 5,000+ arthroscopic procedures.
The Shoulder That Wakes You at Night
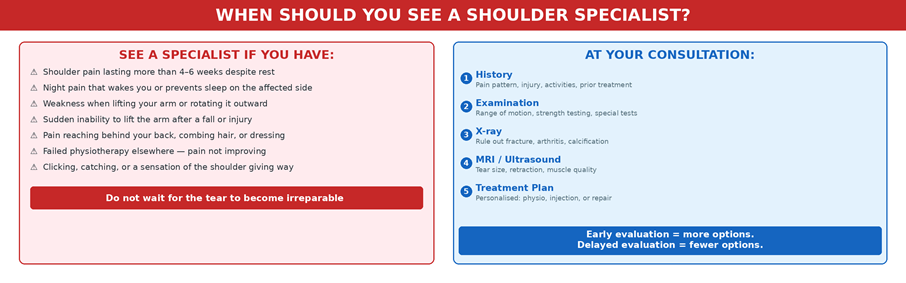
“In my practice at Fortis Mohali, I see patients every day who have been living with shoulder pain for months — sometimes years — before seeking specialist evaluation. They cannot sleep on the affected side. They struggle to comb their hair, put on a shirt, or lift a bucket of water. Some have delayed because they were told the tear would heal on its own. Others delayed because they feared surgery. The reality is this: not every rotator cuff tear needs surgery, but the right tear, left too long, can progress from repairable to irreparable. Early evaluation gives you more options. Delayed evaluation takes options away.”
If you are reading this, you probably have shoulder pain that is not getting better. Perhaps you have been told you have a rotator cuff tear on an MRI or ultrasound. Perhaps you have been doing physiotherapy for weeks and the pain persists. This article is designed to walk you through every treatment option — from rest and rehabilitation to injections and arthroscopic repair — so you can understand when each approach is appropriate, and when it is time to move to the next step.
What Is the Rotator Cuff and Why Does It Tear?
The rotator cuff is a group of four muscles and their tendons — supraspinatus, infraspinatus, subscapularis, and teres minor — that wrap around the head of the humerus (the upper arm bone) like a sleeve. Together, they stabilise the shoulder joint and power the movements we take for granted: lifting the arm, rotating it, reaching overhead, and reaching behind the back. The supraspinatus tendon is the most commonly injured. It runs through a narrow space between the humeral head and the acromion (the bony roof of the shoulder), and it bears the greatest mechanical load during overhead activity.
What Causes Rotator Cuff Tears?
Degenerative tears are by far the most common. The tendon weakens with age, reduced blood supply, and repetitive microtrauma — particularly in people who do overhead work (painters, carpenters, electricians), athletes (badminton, cricket, swimming, volleyball), or those with poor posture and weak scapular muscles. Most tears I see in patients over 50 are degenerative in nature.
Traumatic tears occur suddenly — a fall on an outstretched hand, a heavy lifting injury, or a shoulder dislocation. These are more common in younger, active patients, and the clinical picture is dramatic: sudden inability to lift the arm, immediate weakness, and pain. Traumatic tears in young patients generally need early surgical evaluation because the tendon is healthy — it just needs to be reattached before it retracts.
In North India specifically, I see a high proportion of patients with diabetes-related tendon degeneration, occupational overhead strain (farming, construction), and sports injuries from cricket, kabaddi, and gym training. Diabetes impairs tendon healing and is a risk factor for both developing a tear and for slower post-operative recovery — something that must be factored into every treatment decision.
Symptoms That May Suggest a Rotator Cuff Tear
Rotator cuff tears do not always announce themselves dramatically. Many patients live with a partial tear for months, attributing the pain to “just a sprain” or “age-related stiffness.” The following symptoms should prompt specialist evaluation:
- Pain at night — particularly when lying on the affected shoulder, often waking you from sleep
- A deep, dull ache in the shoulder that worsens with activity and persists at rest
- Weakness when lifting the arm, rotating it outward, or reaching overhead
- Difficulty with everyday tasks: combing hair, putting on a shirt, reaching behind the back, lifting a kettle
- A crackling or catching sensation (crepitus) when moving the shoulder
- Sudden inability to lift the arm after a fall, a pull, or a heavy lift — this suggests an acute tear and requires urgent evaluation
How Rotator Cuff Problems Are Diagnosed
At your first consultation, I take a detailed history — when the pain started, what makes it worse, what you have tried so far, your occupation, sports, and daily demands. The physical examination includes range of motion testing, strength testing of each rotator cuff muscle, and specific clinical tests (Jobe’s test, external rotation lag sign, lift-off test) that help identify which tendon is involved.
An X-ray is usually the first imaging study — it does not show the tendon itself, but it rules out fractures, arthritis, and calcification, and shows the shape of the acromion (a hooked acromion can impinge on the tendon). An MRI or high-resolution ultrasound is the definitive imaging study. It shows the tear size, the degree of tendon retraction from the bone, and critically, the quality of the muscle — whether it has developed fatty infiltration (muscle turning to fat), which is the key factor in determining whether a tear is repairable.
“The MRI does not just show me the tear. It tells me whether we are early enough to repair it. Once fatty infiltration progresses beyond a certain point, the muscle no longer functions even if the tendon is surgically reattached. This is why timing matters.”
Rotator Cuff Treatment Options: A Step-by-Step Approach
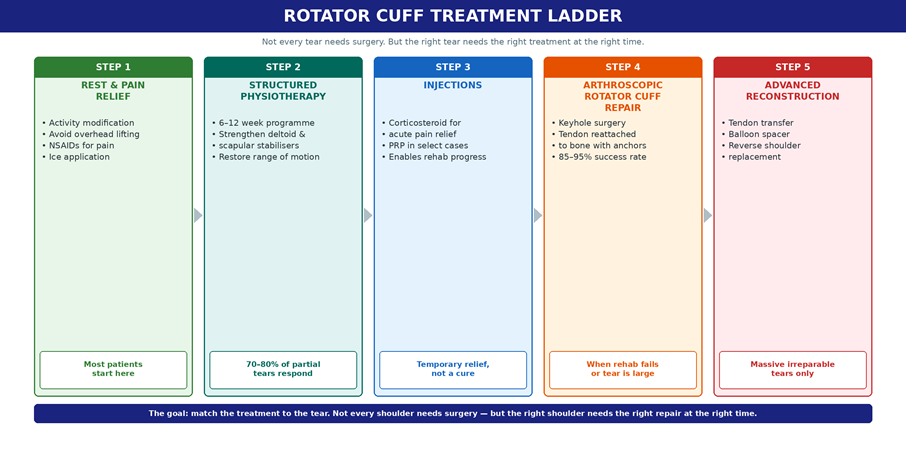
Not every rotator cuff tear needs surgery. But not every tear should be left to physiotherapy forever either. The key is matching the right treatment to the right tear at the right time. Here is the treatment ladder I follow in my practice, consistent with current AAOS Clinical Practice Guidelines.
Step 1: Rest, Activity Modification, and Pain Relief
The first step for most patients is simple: stop doing the things that make the shoulder worse. Avoid overhead lifting, repetitive reaching, and sleeping on the affected side. Over-the-counter anti-inflammatory medications (NSAIDs) can help reduce pain and inflammation in the short term. Ice application after activity provides symptom relief. This phase is appropriate for patients with mild symptoms, early tendinopathy (inflammation without a structural tear), and as a starting point before formal rehabilitation.
Step 2: Structured Physiotherapy
Physiotherapy is the first-line specialist treatment for many rotator cuff problems, and I cannot overstate its importance. A well-designed 6–12 week programme focuses on strengthening the deltoid and scapular stabiliser muscles (which compensate for a weakened rotator cuff), restoring range of motion, correcting shoulder mechanics, and gradually reintroducing functional activities.
For partial-thickness tears, tendinopathy, and small degenerative tears in lower-demand patients, structured physiotherapy is often sufficient. Published evidence suggests that 70–80% of partial tears respond well to rehabilitation. The AAOS guidelines confirm that for small to medium full-thickness tears, both physical therapy and surgery can significantly improve outcomes — meaning physiotherapy is not just a placeholder while waiting for surgery. It is a valid treatment in its own right.
However, physiotherapy has limits. If pain persists after 3–6 months of structured rehabilitation, if weakness is not improving, or if imaging shows the tear is enlarging, it is time to reassess.
Step 3: Injections — A Bridge, Not a Cure
Corticosteroid injections into the subacromial space can provide significant short-term pain relief, particularly when pain is severe enough to prevent the patient from participating in physiotherapy. They reduce inflammation and break the pain cycle, creating a window for rehabilitation to work. However, they are not a cure for a torn tendon, and their use must be carefully timed — the AAOS notes that steroid injections given too close to surgical repair may impair tendon healing.
Platelet-rich plasma (PRP) injections are used in select cases, particularly for partial tears and tendinopathy, where the growth factors in PRP may support biological healing. The evidence is still evolving, and I discuss the realistic expectations with each patient.
Step 4: When Surgery Becomes the Right Answer
This is the critical decision point. Surgery is not the first line of defence, but delaying it when it is needed leads to consequences that cannot be reversed.
I recommend surgical evaluation when:
- Pain persists despite 3–6 months of structured physiotherapy and the patient’s quality of life is significantly affected
- Night pain continues to disrupt sleep despite conservative measures
- There is measurable weakness — the patient cannot lift their arm against resistance, or strength testing shows a clear deficit
- The tear is full-thickness and the patient is active, with functional demands that a torn tendon cannot meet
- The tear is traumatic (acute injury in a younger patient) — early repair gives the best results because the tendon is healthy
- Follow-up imaging shows the tear is enlarging, or muscle quality is deteriorating (fatty infiltration progressing)
The risk of delaying surgery when it is indicated is real and measurable. Over time, a torn tendon retracts away from the bone. The muscle it is attached to shortens and develops fatty infiltration — muscle literally turns to fat. Once fatty infiltration progresses beyond a certain stage, the tendon can be surgically reattached but the muscle can no longer function. The repair has been done, but the shoulder does not get stronger. This is why I tell patients: early evaluation gives you more options. Delayed evaluation takes options away.
Arthroscopic Rotator Cuff Repair: What Happens in Surgery
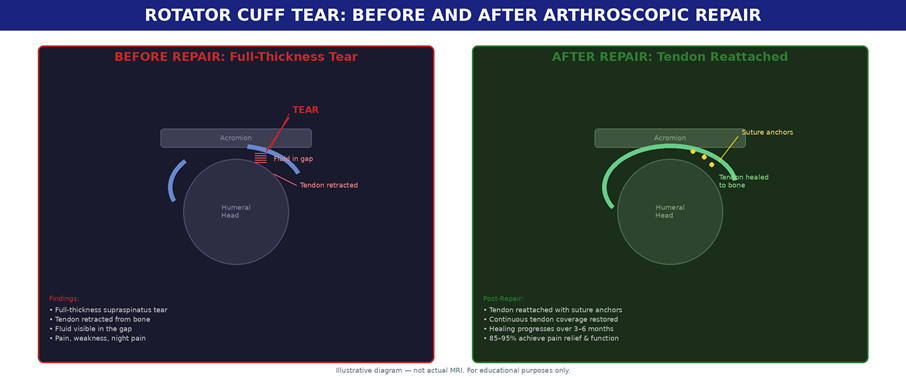
Arthroscopic rotator cuff repair is the gold standard for surgical treatment. It is a keyhole procedure performed through 3–4 small incisions (each about 5–8 mm), using a high-definition camera and specialised instruments. The torn tendon is mobilised, prepared, and reattached to its original footprint on the humeral head using biocompatible suture anchors — small devices that are drilled into the bone and hold the tendon in place while it heals.
In my practice, I use a double-row suture anchor technique for larger tears, which distributes the repair force across a wider area and improves healing rates. Where indicated, I perform concomitant procedures in the same sitting — acromioplasty (shaving the underside of the acromion to create more space for the tendon), biceps tenodesis (addressing a damaged long head of biceps tendon), or SLAP repair (fixing a torn labrum at the top of the socket).
The advantages of arthroscopic over traditional open surgery are significant: smaller incisions, less post-operative pain, lower infection risk, better visualisation of the tear, and faster early rehabilitation. Published outcomes show 85–95% of appropriately selected patients achieve meaningful pain relief and functional improvement after arthroscopic rotator cuff repair.
From the Practice: A Case That Illustrates the Decision
“A 48-year-old badminton player from Chandigarh came to me after six months of worsening shoulder pain. He had tried physiotherapy, two steroid injections, and rest — but he could no longer serve overhead, and night pain was waking him every night. MRI showed a full-thickness supraspinatus tear with early retraction but no significant fatty infiltration — meaning we were still within the window for a good repair. We performed an arthroscopic double-row repair. He was in a sling for five weeks, started guided rehabilitation at week six, and was back playing competitive badminton at five months. Had he waited another year, the muscle quality would have deteriorated and the outcome would have been significantly worse.”
Recovery After Rotator Cuff Repair: What to Expect
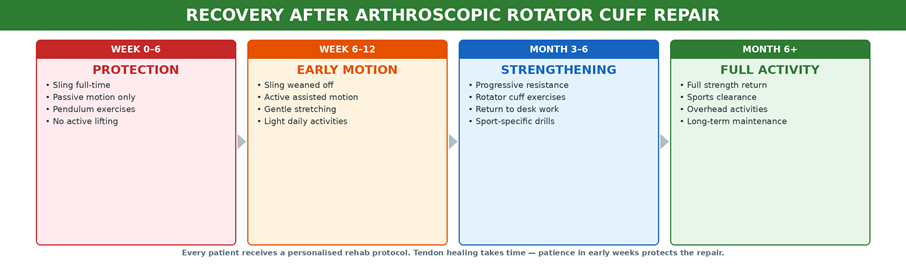
Recovery from rotator cuff repair requires patience. The tendon takes 3–6 months to biologically heal to bone. Pushing too hard, too early, is the single most common reason for repair failure. Every patient at Fortis Mohali receives a personalised rehabilitation protocol that I design in collaboration with our in-house sports physiotherapy team.
Weeks 0–6 (Protection Phase): The arm is in a sling full-time. Only passive movements (performed by the physiotherapist, not the patient) are allowed. Pendulum exercises begin within the first week to prevent stiffness. No active lifting, no driving, no reaching.
Weeks 6–12 (Early Motion Phase): The sling is gradually weaned off. Active-assisted motion begins — the patient starts using the shoulder with gentle guidance. Light daily activities resume. The tendon is healing but not yet strong enough for loading.
Months 3–6 (Strengthening Phase): Progressive resistance exercises begin. Rotator cuff and scapular strengthening. Return to desk work and light activities. Sport-specific drills begin for athletes. This is where the shoulder starts to feel genuinely strong again.
Month 6+ (Full Activity): Most patients achieve 80–90% of their pre-injury strength. Sports clearance is given based on strength testing and functional assessment. Overhead activities, gym, and contact sports are progressively reintroduced. Long-term maintenance exercises continue to protect the repair.
When the Tear Is Irreparable: Advanced Options
In some cases — typically massive tears that have been present for years, with significant tendon retraction and advanced fatty infiltration — the tear cannot be repaired. The tendon is beyond the point where reattachment would be meaningful. This is why early evaluation matters so much. For these patients, I discuss advanced reconstruction options:
Subacromial balloon spacer: A biodegradable balloon is arthroscopically inserted into the subacromial space. It acts as a cushion, pushing the humeral head down and restoring the biomechanical fulcrum so the deltoid can compensate for the absent rotator cuff. The balloon degrades over 12 months, by which time the surrounding tissue has adapted. This is a less invasive option that can significantly improve pain and function in appropriately selected patients.
Tendon transfer: A nearby healthy tendon (typically the latissimus dorsi or lower trapezius) is rerouted to take over the function of the irreparable rotator cuff tendon. This is a more complex procedure but can restore meaningful function in younger, active patients.
Reverse shoulder replacement: For patients with a massive irreparable tear combined with shoulder arthritis (cuff tear arthropathy), reverse shoulder arthroplasty changes the biomechanics of the joint entirely — placing the ball on the scapula side and the socket on the humerus side — allowing the deltoid to power the shoulder without a functioning rotator cuff. This is the definitive solution when all other options have been exhausted.
Why Specialist Decision-Making Matters
The difference between a good outcome and a poor one in rotator cuff disease often comes down to the accuracy of the initial decision: which tears to rehabilitate, which to inject, and which to repair — and when. This requires a surgeon who treats shoulders as a primary focus, not an occasional case among a general orthopaedic workload.
At Fortis Mohali, the shoulder arthroscopy programme is supported by high-definition 4K arthroscopy towers, specialised shoulder positioning tables, Class 100 laminar flow operating theatres, an in-house sports physiotherapy team that works directly with me on post-operative rehabilitation, and an anaesthesia team experienced in interscalene nerve blocks for superior post-operative pain control. The infrastructure matters — but the decision-making matters more.
Take the Next Step
If your shoulder pain is not improving with rest and physiotherapy, or if weakness and night pain are worsening, a specialist evaluation can clarify whether continued rehabilitation or rotator cuff repair is the better next step. Dr Manit Arora evaluates rotator cuff injuries at Fortis Hospital Mohali with a stepwise, evidence-based approach tailored to the tear pattern, age, activity level, and functional goals of each patient. Bring your previous MRI or ultrasound reports for a comprehensive review.
About the Author
Dr Manit Arora is a Senior Consultant in Orthopaedics and Sports Medicine at Fortis Hospital, Mohali. An Australian-trained orthopaedic and sports medicine surgeon, he holds international fellowships in shoulder and knee arthroscopy from Australia, France, Japan, and the USA. Dr Arora’s sub-specialty focus is shoulder and upper limb surgery, including arthroscopic rotator cuff repair, instability surgery, SLAP repair, and complex shoulder reconstruction. He has performed over 5,000 arthroscopic procedures and serves as visiting faculty at AIIMS Rishikesh and IIM Rohtak. He is a member of the Indian Orthopaedic Association and the Shoulder Society of India. Dr Arora’s patient base spans Chandigarh, Mohali, Panchkula, and across Punjab, Haryana, and Himachal Pradesh.
Contact Us – Fortis Hospital Mohali
For appointments, consultations, and diagnostic services, please contact:
📞 72728 72728
Our care team will assist you with:
Doctor appointments
Diagnostic and screening services
Health check-ups
Call now to book your appointment at Fortis Hospital, Mohali.
Categories
Clear allMeet the doctor

- Orthopaedics | Orthopaedics | Sports Medicine
-
 15 Years
15 Years
-
 550
550
Related Blogs
View all







FAQs
Can a rotator cuff tear heal without surgery?
Partial tears and small degenerative tears can often be managed successfully with structured physiotherapy. The tendon itself does not “heal” in the sense of reattaching to bone, but strengthening the surrounding muscles can compensate for the tear and restore pain-free function. However, larger tears, traumatic tears, and tears with progressive weakness generally require surgical repair for a durable outcome.
How long should I try physiotherapy before considering surgery?
The standard recommendation is 3–6 months of structured, supervised physiotherapy. If pain, weakness, and functional limitation persist despite compliant rehabilitation, it is time to discuss surgical options. Do not wait indefinitely — the longer a full-thickness tear goes unrepaired, the greater the risk of irreversible muscle changes.
Is arthroscopic rotator cuff repair painful?
The procedure is performed under general anaesthesia with an interscalene nerve block that provides 12–24 hours of post-operative pain relief. Most patients describe the first 48–72 hours as uncomfortable but manageable with prescribed medications. The keyhole incisions are small and heal quickly. By two weeks, most patients are comfortable enough to manage daily activities with the unaffected arm.
When can I drive after rotator cuff surgery?
Most patients can resume driving an automatic car at 6–8 weeks, once the sling is removed and active motion has been restored. Driving a manual transmission takes longer because of the gear-shift arm. I assess each patient individually before clearing them to drive.
When can I return to sports after rotator cuff repair?
Non-contact sports (swimming, badminton, golf) are typically cleared at 5–6 months. Contact sports and heavy overhead sports may take 6–9 months. Return to sport is based on objective strength testing and functional assessment, not on a calendar date.
What happens if I leave a full-thickness tear untreated?
A full-thickness tear does not heal on its own. Over time, the tendon retracts further from the bone, the muscle shortens and develops fatty infiltration, and the tear may enlarge. These changes are progressive and largely irreversible. A tear that is repairable today may become irreparable in 12–18 months. This is the strongest argument for timely specialist evaluation — not necessarily immediate surgery, but informed decision-making while options still exist.
What is the success rate of arthroscopic rotator cuff repair?
In appropriately selected patients, published outcomes show 85–95% achieve meaningful pain relief and functional improvement. Success depends on tear size, tissue quality, patient age, diabetes status, and compliance with post-operative rehabilitation. Smaller tears repaired early with good muscle quality have the best outcomes.

Keep track of your appointments, get updates & more!

