





Centre of Excellence for Advanced Minimally Invasive Foot and Ankle Surgery
Fortis Hospital Mohali
Northern India's pioneering subspecialty centre for foot and ankle disorders and advanced foot and ankle surgery in Mohali at Fortis Hospital Mohali transforms patient care where specialized options have been scarce. Every step—walking, running, jumping, dancing—relies on the feet and ankles' intricate biomechanics comprising 26 bones per foot, 33 coordinated joints, over 100 muscles, tendons, and ligaments. Yet problems in these structures often mean limited access to expertise, prolonged recoveries, and outcomes failing to restore normal function Led exclusively by Dr. Chandan Narang, a dedicated foot and ankle surgeon in Mohali whose entire practice focuses solely on foot and ankle conditions—a rarity in India—this Centre of Excellence delivers surgical precision, deep biomechanical understanding, consistent functional results, and mastery over the most challenging cases. As North India's first to systematically introduce minimally invasive surgery (MIS) for complex, high-risk conditions, we convert deformities once needing 2-4 staged surgeries over months into single-stage procedures with minimal tissue trauma, accelerating recovery dramatically.
The Critical Need for Dedicated Foot & Ankle Subspecialty Care
Foot and ankle pathology defies comparison with other musculoskeletal areas due to extreme complexity. Biomechanically, each foot manages full body weight through intricate stability-mobility balance, where even minor misalignments trigger cascading disabilities affecting gait, balance, and quality of life. The soft tissue envelope poses unique risks: thin skin with minimal subcutaneous padding, variable blood supply (worse in hindfoot), and scarring potential that compromises vascularity and motion. High-risk populations amplify challenges—diabetics with neuropathy and poor healing, neurological patients with spasticity/imbalance, post-burn/trauma cases with scarred coverage, and athletes demanding rapid performance return.
General orthopedic surgeons, handling diverse anatomy, perform hundreds of foot-ankle procedures lifetime versus subspecialists' thousands, yielding measurably inferior outcomes: 30-40% higher complications in complex cases, lower AOFAS functional scores, more revisions, prolonged immobilization, and multi-staging where single procedures suffice. Dr. Narang's 100% devotion—uncommon regionally—enables nuanced management of biomechanics unique to this area, rare pathologies like Charcot-Marie-Tooth, and innovations like single-stage MIS corrections for post-stroke deformities. This exclusive focus translates to superior precision, fewer wound issues (critical for thin envelopes), and optimized rehab protocols enabling day-1 walking in select cases.
Minimally Invasive Surgery (MIS): A True Game-Changer
Traditional open foot-ankle surgery mandates large 5-15cm incisions exposing bones/joints, a contrast to modern foot and ankle surgery in Mohali using minimally invasive techniques at Fortis Hospital Mohali. Fortis Mohali's MIS revolution eliminates these through pinhole techniques.
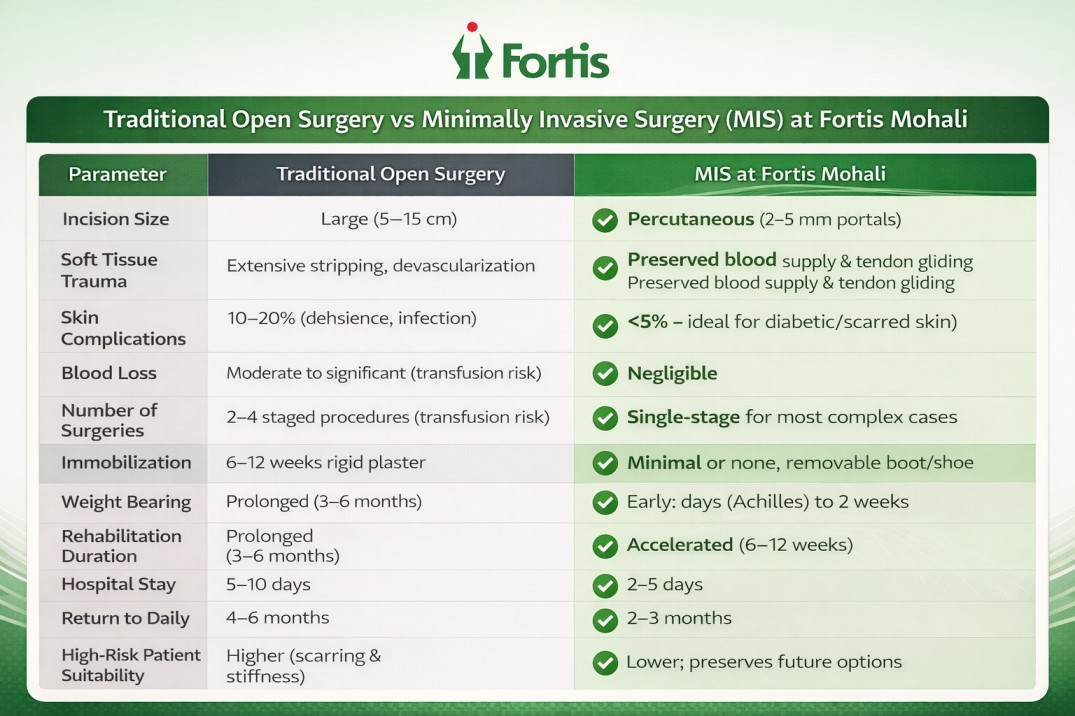
How MIS Works in Practice: Percutaneous osteotomies use specialized burrs/kirschner wires through 2-5mm incisions, guided by intraoperative fluoroscopy for millimeter precision without field exposure. Tendon procedures—releases, lengthenings, transfers—employ small portals preserving paratenon vascularity for faster healing. Soft tissue techniques minimize disruption, crucial for burn/trauma patients. Real-world impact: Post-stroke equinovarus (foot inward/downward, claw toes) traditionally requires Stage 1: soft tissue releases (6 weeks), Stage 2: bone realignment (8 weeks), Stage 3: tendon transfers (6 weeks)—total 6-9 months, 3 surgeries, 30-40% complication risk. MIS: single 2-hour procedure combining all, partial weight-bearing week 1, full gait by 2-3 months.
Comprehensive Spectrum of Conditions Treated
1. Neurological & Post-Burn Deformities
Conditions: Post-stroke equinovarus (spastic inversion, toe clawing), spinal cord injury paralytics, spine fracture sequelae (footdrop, cavovarus), burn contractures (toe webbing, scarred equinus), post-traumatic malunions with compromised envelopes.
Challenges: Severe muscle imbalance, fragile/scarred skin prone to breakdown, infection risks 3x higher, traditional multi-staging impractical.
MIS Solution: Fluoroscopy-guided osteotomies realign bones; percutaneous tenotomies/transfers (e.g., tibialis posterior to peroneals) rebalance; single-stage execution. Outcomes: 3-4 surgeries over 6-12 months → one procedure; early mobilization prevents contracture recurrence; skin preservation vital for burns.
2. Sports Injuries with Accelerated Protocols
Conditions: Achilles acute ruptures/chronic tendinopathy, lateral ankle instability (ATFL/CFL laxity), peroneal/posterior tibial tears, stress/avulsions, osteochondral talar defects.
Traditional Limits: 6-week casts → atrophy, 4-6 month sport returns, re-rupture 10-15%.
Protocol: MIS anatomic repairs (e.g., percutaneous Achilles endobuttons), functional bracing, day-1 walking (select cases), proprioception from week 2. Athlete Results: Professional returns 2-4 months vs. 6; strength 95%+ normalcy.
2A. Specialized Ankle Arthroscopy
Regional rarity: 2-3mm portals with 4mm camera for impingement (anterior/posterior spurs), talar OCDs (microfracture/drilling), instability (ligament debridement), synovitis, loose bodies, early OA. Advantages: Outpatient, days-to-walking, <1% infection, pristine cosmesis vs. open arthrotomy.
3. Bunion & Lesser Toe Deformities
Hallux Valgus/Hammer/Claw/Mallet/Overlapping: MIS chevron/Akin osteotomies, lateral releases via 2-3mm portals; no plaster, 1-2 week bearing, 6-8 week shoes/normalcy; equivalent alignment, superior cosmetics/recovery vs. open.
4. Foot Drop Tendon Transfer Program
Causes: Stroke/spinal/traumatic peroneal palsy, diabetic neuropathy. Approach: Split anterior tibial transfer or flexor hallucis-to-extensor, stable interference screws, 2-3 week motion, gait retraining. Transformation: Brace-free normal walking, regular shoes.
5. Rare Neuromuscular (Charcot-Marie-Tooth, etc.)
Progressive cavus (high arch, calluses, instability): Staged Jones transfer + osteotomies (calcaneal slide, first metatarsal dorsal closing); MIS variants reduce trauma for weak tissues.
6. Heel Complex (Haglund/Spur/Fasciitis/Achilles Insertional)
Percutaneous Haglund resection, endoscopic plantar release (2 portals), tendinopathy debridement: 7-10 day walking, 6-8 week activities, minimal downtime.
7. Ankle Arthritis & Arthrodesis
End-stage post-traumatic/OA, failed TARs: MIS arthrodesis with deformity correction (e.g., supramalleolar osteotomy + tibiotalocalcaneal screw/plate), early loading via locked constructs; subspecialty alignment cuts non-union <5%.
8. Complex Trauma (Pilon/Talus/Calcaneal/Lisfranc/Malunions)
High-energy pilon (soft-tissue mangled), talus AVN-risk, calcaneal 3D collapse, occult Lisfranc, neglected non-unions: MIS fixation + external fixators, Ilizarov for infections, salvage revisions.
9. Flatfoot Disorders Across Lifespan
Pediatric: Coalition resections, flexible vs. rigid. Adult PTTD I-IV: Early MIS repairs/augmentations; late fusions. Comprehensive staging, revision expertise.
10. Diabetic Foot & Limb Salvage
Neuropathy-vascular-Charcot triad: Rocker-bottom reconstructions, post-osteo deformity fixes, ulcer offloading. Multidisciplinary (endo/vascular/ID/wounds): Major amputation prevention priority.
Complete Patient Journey: First Visit to Full Recovery
Step 1: Comprehensive Evaluation (Day 1)
History detailing onset, progression, priors; targeted exam (gait, alignment, neurovascular); multimodal imaging (weight-bearing X-rays, CT for bones, MRI soft tissues); dynamic gait analysis. Non-surgical options exhausted discussed first.
Step 2: Personalized Treatment Blueprint
Condition/severity/activity-tailored: procedure details, MIS candidacy, timelines (e.g., bunion 6-8 weeks vs. Charcot 6 months), risks/benefits, rehab roadmap, consent.
Step 3: Precision Surgical Intervention
MIS-first (1-3 hours under spinal/GA + catheter analgesia); advanced multimodal pain (blocks, PCA, cryoablation select); 2-5 day stay with physio initiation.
Step 4: Accelerated Rehabilitation Phase
Day 1-2 PT (ROM, edema control); week 1 partial bearing; biweekly follow-ups (X-rays); customized home program.
Step 5: Phased Return to Peak Function
- Work: Desk/left foot 1-2 weeks; desk/right 2-4 weeks (driving); standing 6-12 weeks; manual 8-16 weeks.
- Sports: Low-impact (swim/cycle) 6-8 weeks; moderate (golf/tennis) 3-4 months; high-contact (run/soccer) 4-6 months.
Long-term surveillance prevents recurrence.
When to seek specialized foot and ankle care
Consider subspecialty evaluation with a foot and ankle surgeon in Mohali if you have:
- Pain lasting more than three months or pain affecting sleep and daily activity
- A visible or progressive deformity such as bunion, flat foot collapse, or toe deformities
- Recurrent sprains, instability, or repeated injuries
- Difficulty wearing regular shoes
- Foot drop, toe dragging, or balance problems
- Diabetes with ulcers, deformity, infections, or Charcot changes
- Prior surgery with persistent pain, recurrence, or complications
- Neurological conditions, prior burns, or significant scarring around the foot and ankle
Early evaluation often prevents progression and can reduce the complexity of treatment later.
Frequently asked questions
What makes a foot and ankle subspecialist different from a general orthopaedic surgeon?
Foot and ankle surgery involves distinct biomechanics, deformity patterns, and soft tissue constraints. A subspecialist who focuses exclusively on this region develops deeper technical mastery, more consistent decision making, and greater experience with complex and revision cases.
What is minimally invasive foot and ankle surgery?
MIS uses specialized instruments and techniques to perform corrections through small incisions, reducing soft tissue trauma while achieving precise alignment and stable fixation when required.
Will I need a cast after surgery?
This depends on the procedure. Many MIS procedures use a removable boot or protective shoe instead of prolonged casting. Some reconstructions and fusion procedures still require immobilization for healing.
When can I walk after surgery?
Walking timelines vary by procedure and stability. Some repairs allow very early protected weight bearing. Others require staged progression. Even when full weight bearing is delayed, early motion is often encouraged to reduce stiffness.
How long will I be off work?
Return to work depends on the procedure and your job demands. Desk based work may resume earlier than jobs requiring prolonged standing or manual labour. We provide individualized guidance.
How long until return to sports?
This varies by sport and procedure. Lower impact activities may resume earlier. Running and pivoting sports typically require longer rehabilitation. The centre emphasizes safe progression to reduce re injury risk.
What are the risks of foot and ankle surgery?
Risks include infection, wound problems, nerve irritation, stiffness, recurrence, and delayed bone healing in specific procedures. Patient specific factors like diabetes and smoking increase risk, which is why technique selection and soft tissue preservation matter.
Can failed surgery be corrected?
Revision surgery is often possible, including failed bunion correction, recurrent instability, malunions, non unions, and persistent pain after procedures elsewhere. Revision requires careful analysis of why the initial treatment failed and a customized plan.
Take the next step toward pain free mobility
Whether the issue is a bunion, repeated ankle sprains, chronic heel pain, a deformity after stroke or burn, or a diabetic foot complication, the Centre of Excellence for Advanced and Minimally Invasive Foot and Ankle Surgery at Fortis Hospital Mohali is built to help you return to confident movement.
Contact
Phone: +91 72728 72728
Location : Fortis Hospital Mohali, Sector 62, Phase VIII, Sahibzada Ajit Singh Nagar, Punjab 160062
Categories
Clear allMeet the doctor

- Orthopaedics | Orthopaedics
-
 7 Years
7 Years
-
 1050
1050
Related Blogs
View all








Keep track of your appointments, get updates & more!

