





Decoding Your Cancer’s DNA | Understanding Precision Oncology & Personalised Treatment for Cancer
Understanding Precision Oncology: The Right Treatment for the Right Cancer at the Right Time
The Question That Changed Cancer Medicine
“For decades, oncologists asked one question: where is the cancer? Today, the question that matters most is: what is driving this cancer? The answer changes everything — from which drug we choose, to how well it works, to whether the patient needs chemotherapy at all.”
If you or someone you love has been diagnosed with cancer, you have probably heard terms like “stage,” “grade,” and “type.” These are important. But in 2026, they are no longer enough to make the best treatment decisions. Two patients with the same type and stage of cancer can have completely different outcomes depending on the molecular biology driving their individual tumour — and the treatment that matches it.
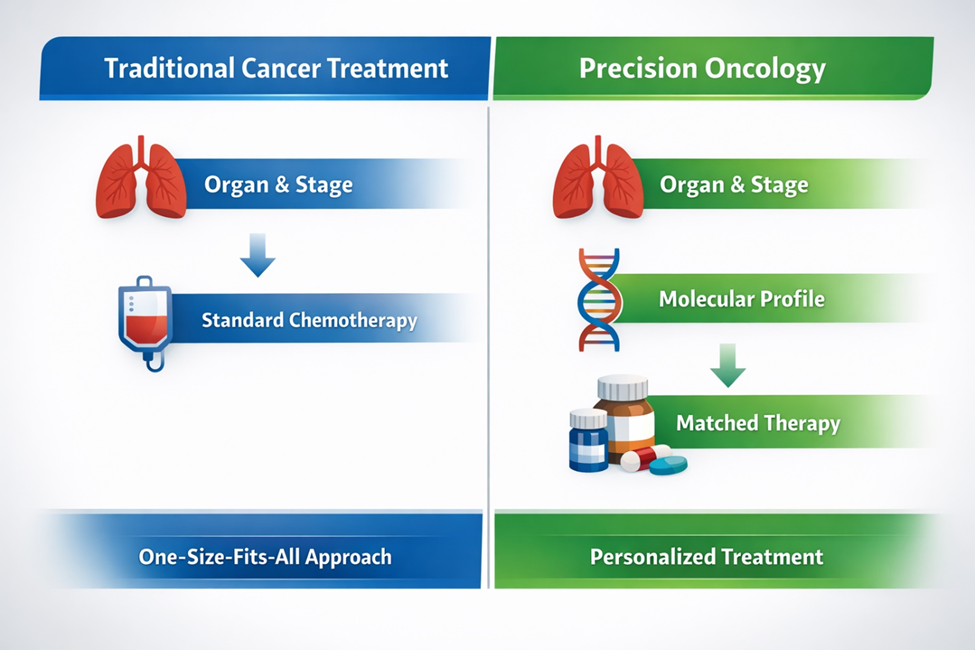
This is the core principle of precision oncology — sometimes called personalised cancer treatment: treating cancer based not only on where it is and how far it has spread, but on the specific genetic mutations and molecular pathways that are fuelling that particular tumour in that particular patient. It is the shift from “one-size-fits-all” to “the right drug for the right target.”
In my 30+ years leading the Department of Medical Oncology at the Fortis Cancer Institute, Mohali, I have seen this evolution transform outcomes for patients across every cancer type — from solid tumours like lung and breast cancer to blood cancers like leukaemia and lymphoma. This article explains what precision oncology means, why it matters for your treatment, and how it works in practice.
From One-Size-Fits-All to Molecularly Guided Therapy
Twenty years ago, cancer treatment was largely determined by the organ of origin. If a patient had lung cancer, they received the standard lung cancer chemotherapy regimen. If they had breast cancer, they received the standard breast protocol. The assumption was that all lung cancers were fundamentally similar, and all breast cancers behaved the same way.
We now know that assumption was wrong. A lung cancer driven by an EGFR mutation (a change in a gene that controls cell growth) behaves entirely differently from one driven by an ALK rearrangement or a KRAS mutation. A breast cancer that overexpresses the HER2 protein (a growth-promoting protein on the surface of cancer cells) requires a completely different treatment strategy than one that is hormone-receptor positive or triple-negative. And a chronic myeloid leukaemia (CML) — a type of blood cancer — driven by the BCR-ABL fusion gene responds dramatically to a specific targeted drug — a discovery that turned a once-fatal disease into a manageable chronic condition.
The difference is not just academic. It determines whether a patient receives a daily oral pill or months of intravenous chemotherapy. It determines whether the treatment targets the cancer precisely or damages healthy cells along the way. It determines response rates, survival, quality of life, and side effects.
Three Patients, Three Cancers, Three Completely Different Treatments
The best way to understand precision oncology is through real examples. Consider three patients, each newly diagnosed, each treated at the same cancer centre, each with a completely different molecular profile and treatment path.
Patient A: Lung Cancer with an EGFR Mutation
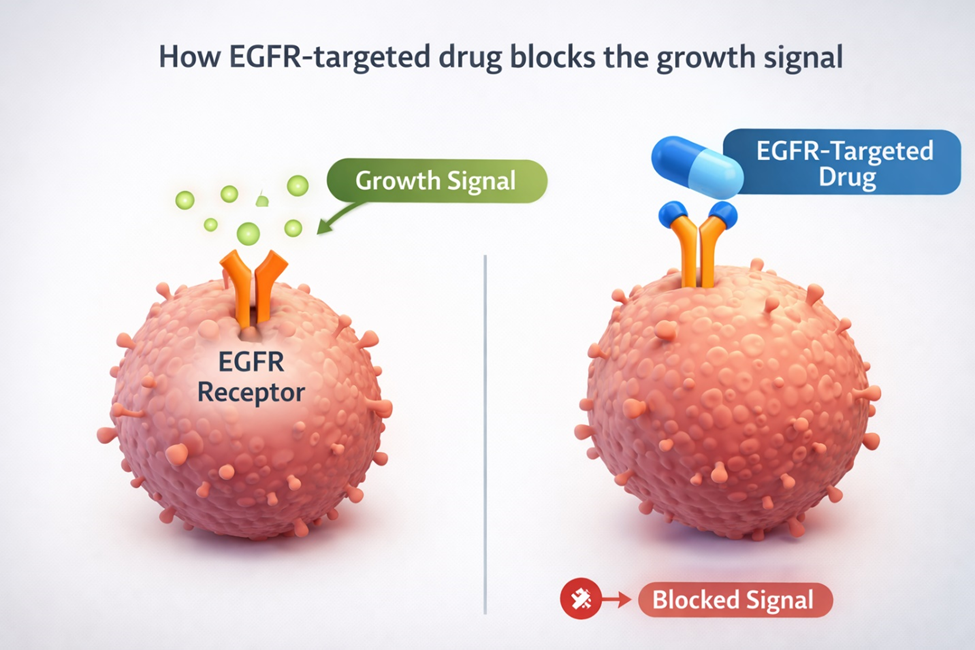
A 55-year-old non-smoker is diagnosed with advanced lung adenocarcinoma (a common type of lung cancer that starts in the mucus-producing cells). In the traditional model, she would receive standard platinum-based chemotherapy. But genomic profiling of her tumour reveals an EGFR exon 19 deletion — a specific mutation that makes the cancer vulnerable to a class of oral targeted drugs called EGFR tyrosine kinase inhibitors. Instead of intravenous chemotherapy with its well-known side effects, she takes a daily pill. Her tumour shrinks significantly within weeks. Her treatment is outpatient, her side effects are manageable, and her quality of life is preserved.
Without molecular profiling, this patient would have received chemotherapy that her cancer was less likely to respond to, with more toxicity and lower efficacy. The mutation was the key that unlocked the right treatment.
Patient B: Breast Cancer That Is HER2-Positive
A 42-year-old woman is diagnosed with invasive breast cancer. Pathology and molecular testing reveal that her tumour overexpresses the HER2 protein — a feature that was once associated with the most aggressive form of breast cancer. Today, HER2-positive breast cancer is one of the most treatable subtypes, thanks to targeted anti-HER2 therapies like trastuzumab and pertuzumab. These drugs, combined with chemotherapy, produce complete pathological response rates that were unimaginable a generation ago.
The same breast cancer without HER2 overexpression would receive a completely different treatment — perhaps hormone therapy alone if it is hormone-receptor positive, or immunotherapy if it is triple-negative with high PD-L1 expression. The molecular profile dictates the entire approach.
Patient C: Chronic Myeloid Leukaemia with BCR-ABL Fusion
A 48-year-old man is diagnosed with chronic myeloid leukaemia (CML). Molecular testing identifies the BCR-ABL fusion gene — the hallmark genetic abnormality of CML. Before the era of precision oncology, CML was often fatal within three to five years, and the only curative option was a bone marrow transplant. Today, oral tyrosine kinase inhibitors like imatinib target the BCR-ABL protein directly, achieving deep molecular remission in the majority of patients. Most CML patients now have near-normal life expectancy on a daily pill, without ever needing chemotherapy or transplant.
This is arguably the single greatest success story in the history of precision oncology — and it illustrates the principle perfectly: when you understand the molecular driver, you can design a treatment that attacks the cancer at its root.

How Precision Oncology Works in Practice
Precision oncology is not a single test or a single drug. It is a workflow — a systematic approach that begins the moment cancer is diagnosed and continues throughout the entire treatment journey.
Step 1: Molecular Profiling — Understanding What Drives the Cancer
When a tumour sample is obtained through biopsy, it undergoes not only standard pathology (which tells us the type and grade of cancer) but also molecular profiling — advanced genomic testing that analyses the tumour’s DNA for specific mutations, fusions, amplifications, and biomarkers. At FCI Mohali, this is coordinated through the Fortis Institute of Genomic Medicine, led by Dr Ravneet Kaur (DM Medical Genetics, AIIMS New Delhi), using next-generation sequencing (NGS), immunohistochemistry panels, and liquid biopsy technology (a blood test that can detect fragments of cancer DNA circulating in the bloodstream).
The profiling identifies actionable targets — the specific molecular vulnerabilities that a targeted drug or immunotherapy can exploit. Not every cancer has an actionable mutation, but when one is found, it can fundamentally change the treatment approach.
Step 2: Tumour Board Review — Where Every Specialist Weighs In
Every cancer case at FCI Mohali is reviewed by the multidisciplinary Tumour Board — a panel that includes medical oncologists, surgical oncologists, radiation oncologists, onco-pathologists, radiologists, nuclear medicine specialists, and medical geneticists. The molecular profiling results are integrated with imaging, pathology, and the patient’s overall clinical picture to develop a personalised treatment plan.
This is not a formality. The Tumour Board may determine that a patient needs targeted therapy before surgery (neoadjuvant) to shrink the tumour. Or that surgery should come first, followed by adjuvant immunotherapy. Or that radiation and systemic therapy should proceed concurrently. The sequence matters as much as the drugs, and only a multidisciplinary discussion can optimise it.
Step 3: Matched Treatment — Targeted Therapy, Immunotherapy, or Chemotherapy
Based on the molecular profile and Tumour Board recommendation, the medical oncologist selects from an expanding arsenal:
Targeted Therapy
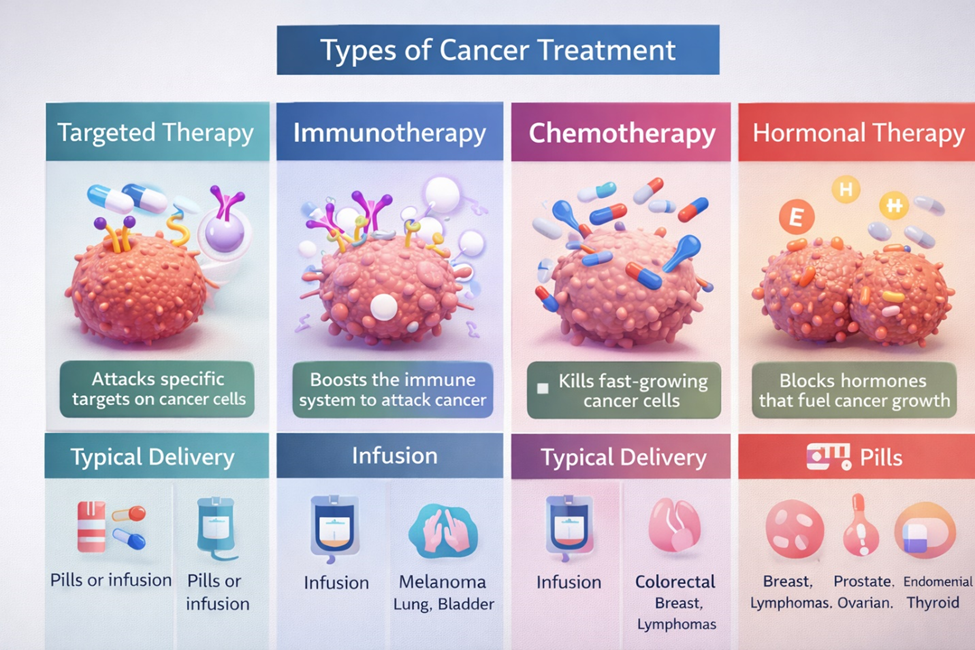
Targeted therapy uses drugs designed to attack specific molecular targets on cancer cells. Examples include EGFR inhibitors for EGFR-mutant lung cancer, ALK inhibitors for ALK-positive lung cancer, anti-HER2 agents for HER2-positive breast cancer, BRAF inhibitors for BRAF-mutant melanoma, and tyrosine kinase inhibitors for BCR-ABL-positive CML. These drugs are often oral, outpatient, and associated with fewer of the traditional chemotherapy side effects.
Immunotherapy
Targeted therapy uses drugs designed to attack specific molecular targets on cancer cells. Examples include EGFR inhibitors for EGFR-mutant lung cancer, distinct oral ALK inhibitor tablets tailored for ALK-positive lung cancer, anti-HER2 agents for HER2-positive breast cancer, BRAF inhibitors for BRAF-mutant melanoma, and tyrosine kinase inhibitors for BCR-ABL-positive CML. These drugs are often convenient, outpatient oral treatments associated with fewer of the traditional chemotherapy side effects.
Chemotherapy
Chemotherapy remains an essential and effective tool — but in the precision era, it is no longer the default for every patient. When chemotherapy is needed, it is often combined with targeted or immune agents for synergistic effect, or used in dose-dense protocols that shorten treatment duration. Modern supportive care (anti-nausea drugs, growth factors, fertility preservation) has dramatically improved tolerability.
Hormonal Therapy
Hormonal therapy is a cornerstone for hormone-receptor-positive breast cancer and prostate cancer, often combined with CDK4/6 inhibitors or newer androgen-pathway agents to improve outcomes.
Step 4: Monitoring, Adaptation, and Response Assessment
Precision oncology does not stop once treatment begins. Tumour response is monitored through imaging and, increasingly, through liquid biopsy — a blood test that detects circulating tumour DNA to track treatment response in real time and identify emerging resistance mutations before they become clinically apparent. If the cancer develops resistance to a targeted agent, re-profiling the tumour can reveal new mutations that a second-line targeted drug can exploit. Treatment adapts as the cancer evolves.
What This Means for You as a Patient
If you have been diagnosed with cancer, precision oncology means that your treatment plan will be built around your specific disease, not a generic protocol. It means your tumour’s molecular profile will be analysed to identify whether a targeted drug or immunotherapy could work better than standard chemotherapy. It means that every decision will be made by a multidisciplinary team, not a single doctor acting alone. And it means that if your cancer changes over time, your treatment can adapt with it.
Not every cancer has an actionable molecular target — and it is important to be honest about that. For some patients, chemotherapy remains the best and most effective option. But even in those cases, molecular profiling provides valuable information: it may reveal that immunotherapy should be added, or that a specific combination regimen will work better, or that the cancer is unlikely to respond to a particular drug, sparing the patient unnecessary toxicity.
The goal is always the same: maximum cancer control with minimum impact on your quality of life. Precision oncology gives us more tools to achieve that goal than at any point in the history of cancer medicine.
Why Fortis Cancer Institute, Mohali
Precision oncology requires more than a good oncologist. It requires an ecosystem: genomic testing capabilities, a functional Tumour Board, organ-specific surgical specialists, an advanced radiation platform, and supportive care services — all working together under one roof.
- The Fortis Institute of Genomic Medicine provides next-generation sequencing, hereditary cancer testing, liquid biopsy, and pharmacogenomics as an integral part of cancer care.
- Every case is reviewed by the multidisciplinary Tumour Board before treatment begins.
- Organ-specific surgical oncologists and robotic surgery (1,200+ procedures, 5 certified proctors) ensure surgical precision.
- The radiation platform includes SGRT, MRI-based brachytherapy with the Geneva applicator, HDRS with 6-degree couch, and 4DCT motion management — the most comprehensive setup north of Delhi.
- Supportive services including pain management, nutrition, psychology, palliative care, and rehabilitation surround the patient at every step.
This integration is what makes precision oncology work in practice — not as a marketing concept, but as a clinical workflow that improves outcomes for real patients every day.
Your Cancer Deserves a Personalised Approach
“The era of treating all cancers the same way is over. Every tumour has a story written in its DNA. Our job is to read that story and use it to guide the most precise, effective, and least harmful treatment possible. That is precision oncology.” — Dr Rajeev Bedi
To schedule a consultation with Dr Rajeev Bedi at the Fortis Cancer Institute, Mohali, contact the Department of Medical Oncology. We welcome second opinions — bring your biopsy
Contact Us – Fortis Hospital Mohali
For appointments, consultations, and diagnostic services, please contact:
📞 72728 72728
Our care team will assist you with:
Doctor appointments
Diagnostic and screening services
Health check-ups
Call now to book your appointment at Fortis Hospital, Mohali.
Categories
Clear allMeet the doctor

- Oncology | Medical Oncology
-
 27 Years
27 Years
-
 2550
2550
Related Blogs
View all









FAQs
What is precision oncology?
Precision oncology is an approach to cancer treatment where therapy is selected based on the specific molecular and genetic characteristics of each patient’s tumour, rather than using a standard protocol based solely on cancer type and stage. It aims to match the right drug to the right target for better outcomes and fewer side effects.
Does every cancer patient need genomic profiling?
Molecular profiling is increasingly recommended for most advanced cancers, particularly lung, breast, colorectal, melanoma, ovarian, and haematological cancers. Your oncologist will determine which tests are appropriate based on your diagnosis, stage, and the likelihood of finding an actionable target.
Will precision oncology replace chemotherapy?
Not entirely. Chemotherapy remains effective and essential for many cancer types. What precision oncology does is identify patients who may benefit more from targeted therapy or immunotherapy — either instead of or in addition to chemotherapy. The goal is to use every tool optimally, not to eliminate any single approach.
Is precision oncology available for blood cancers?
Absolutely. Blood cancers were among the first to benefit from precision medicine. CML (treated with imatinib targeting BCR-ABL), AML (with FLT3 inhibitors), CLL (with BTK inhibitors), and Hodgkin lymphoma (with checkpoint inhibitors) are all examples where molecular understanding has transformed treatment and outcomes.
What is a Tumour Board and why does it matter?
A Tumour Board is a multidisciplinary panel of specialists who review every cancer case together before recommending a treatment plan. It ensures that no single perspective dominates the decision and that the optimal sequence of surgery, radiation, and systemic therapy is determined collaboratively.
How do I know if my cancer has an actionable mutation?
Through molecular profiling — genomic testing of your tumour tissue (and sometimes a blood-based liquid biopsy). This is typically coordinated by your medical oncologist in consultation with a medical geneticist. At FCI Mohali, this is available through the Institute of Genomic Medicine.

Keep track of your appointments, get updates & more!

