






Deep TMS: The Brain Stimulation Technology That Is Changing Mental Health and Addiction Treatment
What Patients and Families Need to Know
By Dr Hardeep Singh Additional Director - Psychiatrist | Fortis Hospital, Mohali
When Medications Are Not Enough
“As a psychiatrist, one of the most difficult conversations I have is telling a patient that we need to try yet another medication. For patients with treatment-resistant depression, OCD, or substance dependence, the options narrow with every failed trial. Deep TMS has given us a genuinely different tool — one that works through a completely different mechanism.”
If you or someone in your family is living with depression, obsessive-compulsive disorder (OCD), or a substance use disorder (addiction) that has not responded adequately to medications and therapy, you are not alone. Approximately one in three patients with major depression and up to 60 percent of patients with OCD do not achieve satisfactory improvement with standard treatments. Relapse rates in substance use disorders remain as high as 60 percent despite available pharmacological and behavioural therapies.
Deep Transcranial Magnetic Stimulation (Deep TMS) represents a fundamentally different approach. Unlike medications that work through your bloodstream and affect the entire body, Deep TMS directly targets the specific brain circuits involved in your condition — without surgery, without anaesthesia, and without the systemic side effects like weight gain or sexual dysfunction that many psychiatric medications cause. Developed in Israel by BrainsWay and based on research originating at the US National Institutes of Health, it uses magnetic fields to stimulate the neural circuits responsible for mood, anxiety, compulsive behaviour, craving, and addiction.
Fortis Hospital Mohali is currently the only centre in the Chandigarh–Mohali–Panchkula region to offer this technology. In this article, I explain what Deep TMS is, how it works, what the evidence says across psychiatric conditions and substance use disorders, and who might benefit.
How Deep TMS Works
Your brain communicates through electrical signals travelling along networks of neurons (brain cells). In depression, certain prefrontal regions (the front part of the brain involved in mood and decision-making) become underactive. In OCD, the medial prefrontal cortex and anterior cingulate show abnormal overactivity — like an alarm that keeps going off even when there’s no danger. In addiction, the prefrontal cortex loses its ability to exert inhibitory control over compulsive drug-seeking behaviour — the brain’s “brake pedal” stops working properly.
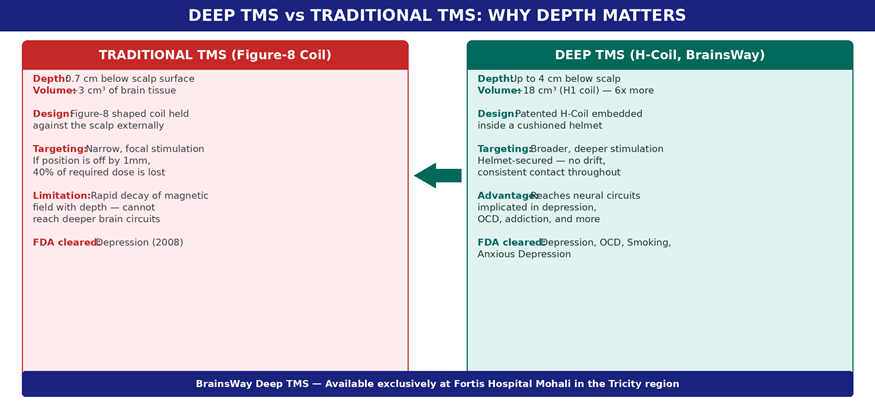
Deep TMS sends brief magnetic pulses through a cushioned helmet into the brain, creating tiny electrical currents that activate or modulate the specific neural circuits implicated in each condition. The patented H-Coil reaches up to 4 cm below the scalp — six times deeper and broader than traditional TMS — allowing it to directly influence circuits that lie beyond the brain’s surface.
Depression: The Strongest Evidence Base
The landmark multicenter randomised controlled trial (Levkovitz et al., World Psychiatry, 2015) demonstrated significant improvement versus sham (a dummy treatment) in patients whose depression had not responded to medications. The most compelling recent data comes from a 2025 post-marketing study of 1,257 adolescents and young adults across 56 sites (Roth et al., Psychiatry Research) — after 36 sessions, the response rate was 75 percent, with median onset at just 13 sessions. These patients had failed an average of 4.5 medications.
For patients across Punjab and the Chandigarh region who have been cycling through antidepressants without adequate relief, these numbers are significant. Deep TMS offers a non-drug pathway that can work alongside existing treatment or, in some cases, reduce the medication burden.
OCD: Targeting the Brain’s Error-Detection Circuit
The H7 Coil targets the medial prefrontal cortex and anterior cingulate cortex — brain regions that drive the intrusive thoughts (“what if I left the gas on?”) and compulsive behaviours (checking, washing, counting) of OCD. A multicenter randomised controlled trial (Carmi et al., American Journal of Psychiatry, 2019) demonstrated significant symptom reduction. Each session includes a brief provocation exposure before stimulation — the therapist deliberately triggers a mild anxiety response to activate the relevant circuits, making them more responsive to modulation by the magnetic pulses.
Substance Use Disorders: A Frontier of Deep TMS
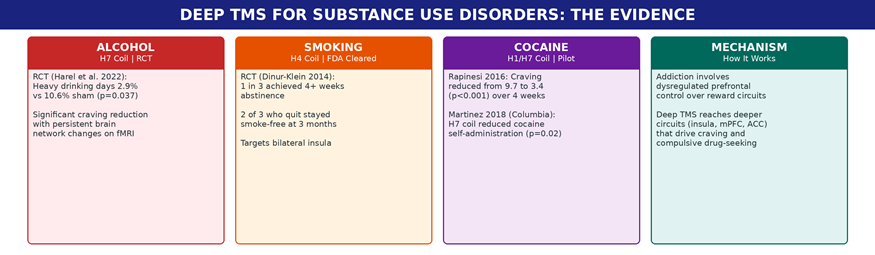
“Addiction is a brain disease, not a moral failing. The prefrontal cortex — the brain’s control centre for decision-making and impulse regulation — becomes dysfunctional in substance dependence. Deep TMS can directly modulate these circuits, offering a tool that addresses the neurobiology of addiction rather than just its symptoms.”
Alcohol Use Disorder
A randomised, double-blind, sham-controlled trial published in Biological Psychiatry (Harel et al., 2022) used the H7 coil to target the medial prefrontal cortex and anterior cingulate cortex in 51 recently abstinent patients with moderate-to-severe alcohol use disorder. The results were striking: heavy drinking days during the 12-week follow-up were 2.9 percent in the active group versus 10.6 percent in sham (p = 0.037). Craving was significantly lower after treatment, and functional MRI showed persistent changes in brain network connectivity — providing a biomarker of genuine neural circuit modulation.
Smoking Cessation
The H4 Coil — which targets the bilateral insula and prefrontal cortex, regions central to craving and interoceptive awareness (the brain’s ability to sense what the body is feeling) — received FDA clearance for smoking cessation in 2020. In the pivotal prospective RCT (Dinur-Klein et al., Biological Psychiatry, 2014), nearly one in three patients who completed treatment achieved four or more weeks of continuous abstinence, and two-thirds of those who quit remained smoke-free at three months. A comprehensive review (Coles et al., American Journal on Addictions, 2018) confirmed that high-frequency stimulation targeting the DLPFC (the outer front part of the brain responsible for self-control) showed the most promising results for tobacco craving reduction across 11 studies.
Cocaine Use Disorder
A pilot study at Sapienza University Rome (Rapinesi et al., Neuroscience Letters, 2016) treated seven patients with cocaine use disorder using add-on Deep TMS to the bilateral DLPFC. Cocaine craving dropped dramatically — from a mean VAS score of 9.7 at baseline to 3.4 after four weeks of treatment (p < 0.001). Craving remained significantly below baseline even four weeks after treatment ended, though it began to increase, suggesting maintenance sessions would be beneficial.
Separately, a pilot study at Columbia University (Martinez et al., Frontiers in Psychiatry, 2018) used the H7 coil targeting the medial prefrontal and anterior cingulate cortices in 18 cocaine-dependent volunteers. High-frequency stimulation significantly reduced cocaine self-administration in a laboratory choice paradigm (p = 0.02), while low-frequency and sham had no effect — demonstrating that Deep TMS can modulate the actual decision to take cocaine, not just subjective craving.
What a Deep TMS Session Looks Like
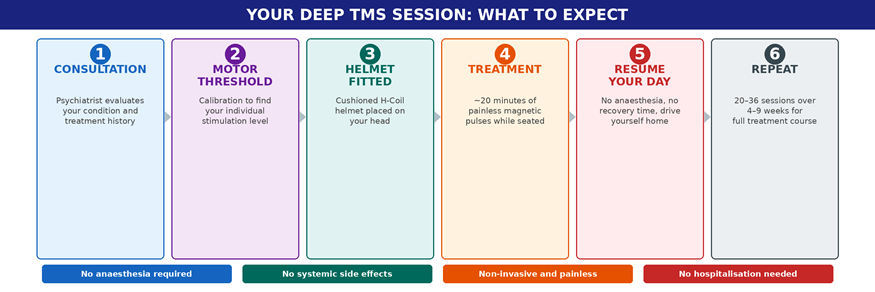
You sit comfortably wearing a cushioned helmet for approximately 20 minutes. You hear clicking sounds and feel a tapping sensation on your scalp, but the procedure is painless. You remain fully awake, require no sedation, and can drive yourself home immediately. A typical course is 20 to 36 sessions over 4 to 9 weeks, depending on the condition being treated.
Safety
Deep TMS has been evaluated in thousands of patients worldwide. The most common side effects are mild scalp discomfort and occasional headache, both of which typically fade within the first few sessions. In the large adolescent study of 1,257 patients, the adverse event rate was very low (headache 0.32%, fatigue 0.24%, one seizure 0.08%). Deep TMS does not cause cognitive side effects (no memory or concentration problems), does not interact with medications, and does not produce systemic effects like weight gain or sexual dysfunction — side effects that lead many patients to stop their psychiatric medications.
Who Should Consider Deep TMS?
- Treatment-resistant depression — if you have tried at least one antidepressant without adequate improvement
- OCD not responding to SSRIs (a class of antidepressant commonly used for OCD) and/or cognitive behavioural therapy (CBT)
- Alcohol use disorder — as an add-on to support abstinence and reduce craving
- Smoking cessation — for patients who have tried nicotine replacement therapy and medications without success
- Patients who experience intolerable side effects from psychiatric medications
- Adolescents and young adults with treatment-resistant depression
- Neurological conditions (Parkinson’s, Alzheimer’s) — see the companion blog by Dr Nishit Sawal
If you are unsure whether Deep TMS might be appropriate for your situation, the first step is a detailed psychiatric evaluation. Not every patient with depression or OCD needs TMS — many respond well to the right combination of medication and therapy. Dr Hardeep Singh’s approach at Fortis Mohali begins with a comprehensive assessment to determine whether Deep TMS is genuinely the right next step, or whether adjusting current treatment would be more appropriate. This matters, because the technology works best when applied to the right patients at the right stage of their treatment journey.
Your Next Step
To schedule a Deep TMS consultation at Fortis Hospital Mohali, contact the Department of Psychiatry. Bring your treatment records, medication history, and any relevant assessments. Patients from across Chandigarh, Panchkula, Punjab, and neighbouring states are welcome — the initial evaluation can help determine whether Deep TMS is the right fit before committing to a treatment course.
About the Author
Dr Hardeep Singh is a Additional Director - Psychiatrist at Fortis Hospital, Mohali, leading the Deep TMS programme — the first and only in the Tricity region. His practice encompasses treatment-resistant depression, anxiety disorders, OCD, and substance use disorders, serving patients across Punjab, Haryana, Himachal Pradesh, and Jammu & Kashmir.
Categories
Clear allMeet the doctor

- Mental Health and Behavioural Sciences | Mental Health and Behavioural Sciences
-
 26 Years
26 Years
-
 2050
2050
Related Blogs
View all
Are We Under Or Over Diagnosing Psychological Issues In Children

Healthy Coping Strategies To Adopt When You Are Overwhelmed By Your Workload

Dealing With Relationships: A Guide For Young People

Asking For Help - Things To Share And Consider When Seeking Help

How Psychological Safety Looks Like At A Workplace

How To Create A Workplace That Motivates Employees To Do Their Best

How To Make A Smooth Transition To A New Job


FAQs
What does Deep TMS feel like?
You feel a tapping or knocking sensation on your scalp and hear clicking sounds during the 20-minute session. Most patients describe it as unusual but not painful. You remain fully awake, can talk, and need no recovery time afterward.
How is Deep TMS different from regular TMS?
Traditional (surface) TMS uses a figure-8 coil that stimulates about 1.5 cm into the brain. Deep TMS uses the patented H-Coil, which reaches up to 4 cm deep and stimulates a broader area. This allows it to target deeper brain circuits involved in OCD, addiction, and other conditions beyond depression.
Can I continue my medications during Deep TMS?
Yes. Deep TMS does not interact with psychiatric medications. Many patients continue their existing prescriptions during treatment. In some cases, medications can be adjusted or reduced after a successful TMS course, under your psychiatrist’s guidance.
Is Deep TMS safe for teenagers?
The 2025 post-marketing study of 1,257 adolescents and young adults showed Deep TMS to be well-tolerated with very low adverse event rates. It is increasingly used for treatment-resistant depression in younger patients when medications have not worked.
Does insurance cover Deep TMS in India?
Coverage varies by insurance provider and policy. The team at Fortis Mohali can help you check your eligibility and provide transparent cost estimates before you begin treatment.
Where is Deep TMS available near Chandigarh?
Fortis Hospital Mohali is currently the only centre in the Chandigarh–Mohali–Panchkula Tricity region offering BrainsWay Deep TMS technology. You can schedule a consultation with Dr Hardeep Singh through the Department of Psychiatry.

Keep track of your appointments, get updates & more!

