





Deep TMS for Parkinsons Disease Alzheimers Disease and Other Neurological Conditions
How Non-Invasive Brain Stimulation Is Opening New Doors in Neurology (2026 Update)
By Dr Nishit Sawal Consultant Neurologist | Fortis Hospital, Mohali DM Neurology | Specialist in Movement Disorders, Stroke & Neuromodulation
KEY TAKEAWAY: Deep TMS (Deep Transcranial Magnetic Stimulation) is a non-invasive, FDA-cleared and CE-marked brain stimulation technology now being used as an add-on therapy in neurology. In Parkinson’s disease, randomised controlled trials show 27% motor improvement and a 73% increase in daily “ON” time. In Alzheimer’s disease, early studies show cognitive improvement in 77% of patients. Fortis Hospital Mohali is the only centre in the Chandigarh–Mohali–Panchkula tricity region to offer this technology.
When Neurological Disease Outpaces Available Treatment
“Parkinson’s disease and Alzheimer’s disease remain two of the greatest challenges in neurology. Our current medications can manage symptoms, but they lose effectiveness over time and do not alter the underlying disease trajectory. Deep TMS offers something genuinely different — a non-invasive way to directly modulate the brain circuits that are dysfunctional in these conditions, improving symptoms that medications alone cannot fully address.” — Dr Nishit Sawal, Consultant Neurologist, Fortis Mohali
For patients living with Parkinson’s disease, the frustration is familiar: levodopa works beautifully at first, then gradually loses its effect. Motor fluctuations increase. The proportion of the day spent in an “OFF” state grows. Non-motor symptoms — depression, cognitive slowing, autonomic dysfunction — accumulate. For patients with Alzheimer’s disease, the trajectory is even more relentless: acetylcholinesterase inhibitors may slow decline modestly, but no oral medication reverses or halts the progression.
Deep Transcranial Magnetic Stimulation (Deep TMS) is not a cure for either condition. But a growing body of evidence — including randomised controlled trials and, as of 2026, accelerated treatment protocols with proven long-term durability — suggests that it can improve specific symptoms, sometimes substantially, by directly stimulating the cortical and subcortical circuits these diseases disrupt. As a neurologist, I find this evidence compelling enough to offer Deep TMS as an add-on therapy at Fortis Mohali, where we are the only centre in the tricity region equipped with this Israeli technology.
What Is Deep TMS, and How Is It Different?
Deep TMS uses a patented electromagnetic “H-Coil” embedded in a cushioned helmet to deliver magnetic pulses that stimulate specific brain circuits. Unlike traditional (figure-8) TMS, which reaches only about 0.7 cm beneath the scalp, the H-Coil reaches up to 4 cm deep and stimulates a brain volume roughly six times larger. This deeper, broader reach is precisely what makes it relevant for neurological conditions, where the dysfunctional circuits often lie beneath the cortical surface. The technology was developed by BrainsWay, based on research originating at the US National Institutes of Health, and is the only TMS platform with multiple FDA-cleared indications backed by pivotal clinical trials.
Deep TMS for Parkinson’s Disease: The Strongest Neurological Evidence
The Randomised Controlled Trial
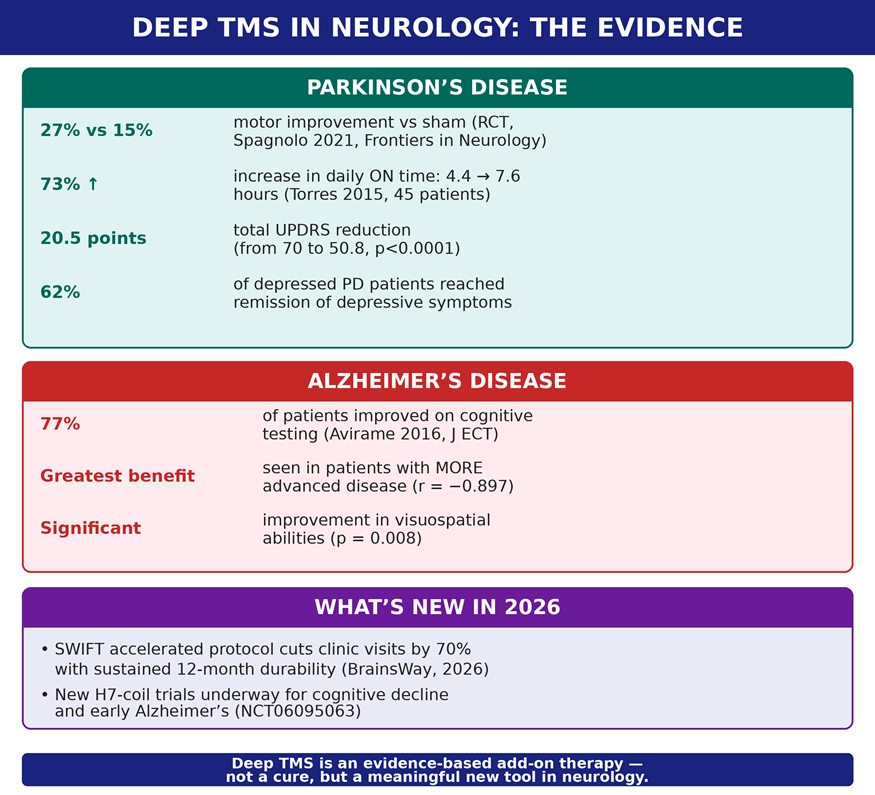
The strongest evidence comes from a double-blind, placebo-controlled, randomised trial conducted at Hospital San Raffaele, Milan (Spagnolo et al., Frontiers in Neurology, 2021). Sixty patients with Parkinson’s disease were randomised to receive real or sham Deep TMS over 12 sessions across four weeks. The results were clear:
- Motor symptoms (UPDRS Part III) improved by 27% in the active group versus 15% with sham (p = 0.007, Cohen’s D = 0.73 — a large effect size).
- Tremor subscore improved significantly in the active group, with almost no change in the sham group (p = 0.011).
- Both the more-affected and less-affected sides of the body showed significant improvement.
- 33 of 39 patients receiving real treatment met criteria for a minimally clinically important improvement.
The Broader Clinical Picture
An earlier study of 45 Parkinson’s disease patients (Torres et al., Frontiers in Neurology, 2015) demonstrated an even wider range of benefits from Deep TMS as an add-on to standard levodopa treatment. Over 14 sessions combining low-frequency motor cortex and high-frequency prefrontal cortex stimulation:
- Total UPDRS score decreased by 20.5 points (from 70 to 50.8; p < 0.0001).
- Gait speed improved significantly on the timed Up & Go test.
- Balance improved on the Tinetti scale, reducing fall risk.
- Depressive symptoms reached remission in 62% of depressed patients.
- Daily “ON” time increased from 4.4 to 7.6 hours — a 73% increase — without any change in medication dosage.
- Autonomic symptoms (cardiovascular, urinary, gastrointestinal) improved significantly.
- Benefits persisted at 30-day follow-up, with some measures continuing to improve after treatment ended.
The breadth of improvement is particularly noteworthy. Standard Parkinson’s treatments address motor symptoms but often leave non-motor symptoms — depression, autonomic dysfunction, gait instability — undertreated. Deep TMS appears to improve the full spectrum, likely because the H-Coil stimulates both the motor cortex and the prefrontal cortex simultaneously, addressing the motor circuitry as well as the mood and autonomic regulatory centres.
Deep TMS for Alzheimer’s Disease: Early but Encouraging
A case series of 11 patients with moderate-to-severe Alzheimer’s disease (Avirame et al., Journal of ECT, 2016) received 20 sessions of high-frequency Deep TMS over the bilateral prefrontal cortex. The results:
- 77% of patients improved on the Addenbrooke’s Cognitive Examination (ACE).
- 60% improved on a computerised cognitive battery (Mindstreams).
- No patient declined on both tests during the treatment period.
- Visuospatial abilities improved significantly (p = 0.008).
- Patients with more advanced disease showed the greatest improvement (r = −0.897, p = 0.001) — suggesting Deep TMS may be most valuable precisely where other treatments have the least to offer.
These findings are preliminary and come from an open-label series without a sham control. However, they are consistent with the broader literature on repetitive TMS in Alzheimer’s disease, where prefrontal stimulation has improved naming, memory retrieval, and executive function. In a condition where the expected trajectory is steady decline, even the preservation of cognitive function over a treatment period is clinically meaningful.
What’s New in 2026: Faster, More Durable Treatment
The Deep TMS field has advanced significantly. In June 2026, BrainsWay presented the first 12-month durability data for its SWIFT accelerated Deep TMS protocol at the Clinical TMS Society Annual Meeting. The SWIFT protocol reduces the number of clinic visits during the acute treatment phase by 70% compared with the standard protocol — condensing weeks of treatment into a much shorter window — while maintaining sustained clinical benefit at one year. For patients travelling long distances to Fortis Mohali from across Punjab, Himachal Pradesh, and Jammu & Kashmir, accelerated protocols have the potential to make treatment far more accessible.
On the neurological frontier specifically, new trials are now underway using the H7-coil Deep TMS system for subjective cognitive decline and early Alzheimer’s disease (ClinicalTrials.gov NCT06095063), reflecting growing scientific interest in whether Deep TMS can intervene earlier in the cognitive decline trajectory — before significant neuronal loss has occurred. Research into Deep TMS for additional neurological applications, including post-stroke rehabilitation, multiple sclerosis-related fatigue, and chronic pain, also continues to expand.
Important context: Deep TMS is one of several neuromodulation approaches being studied in neurology. It is non-invasive (no surgery), distinguishing it from deep brain stimulation (DBS), which requires surgically implanted electrodes. For appropriate patients, Deep TMS offers a lower-risk, outpatient option.
Why Deep TMS Works in Neurological Conditions
In Parkinson’s disease, the dysfunction extends far beyond the dopamine-producing neurons of the substantia nigra. Cortical excitability is impaired, communication between the brain’s hemispheres is disrupted, and the prefrontal-striatal circuits that regulate mood, motivation, and autonomic function are compromised. Deep TMS addresses this by stimulating the motor cortex bilaterally (improving motor symptoms) and the prefrontal cortex (improving mood and non-motor symptoms). Evidence suggests prefrontal stimulation may also enhance the brain’s own dopamine release through cortico-striatal pathways, potentially working in synergy with levodopa.
In Alzheimer’s disease, functional brain-imaging studies show progressive disconnection within the default-mode network and reduced activity in prefrontal regions. Deep TMS may activate frontal “cognitive reserve” circuits and strengthen communication between brain regions, partially compensating for the structural losses in the temporal lobe that underlie memory decline.
What Patients and Families Should Know
Deep TMS for neurological conditions is not a replacement for your current medications. It is an add-on therapy — designed to be used alongside levodopa (for Parkinson’s) or acetylcholinesterase inhibitors (for Alzheimer’s) to enhance their effects and address symptoms they cannot fully control.
The treatment itself is the same non-invasive, outpatient procedure described in the companion blog by Dr Hardeep Singh: a cushioned helmet, approximately 20 minutes per session, no anaesthesia, no sedation, no recovery time, and no systemic side effects. You remain fully awake and can drive yourself home immediately afterward. The specific H-Coil used and the stimulation parameters are tailored to the neurological condition being treated.
The Neurology of Tomorrow, Available Today
“Non-invasive brain stimulation is not science fiction. It is a clinical reality backed by randomised controlled trials and, increasingly, long-term durability data. For my patients with Parkinson’s disease who are losing ON time, or families watching Alzheimer’s take away a loved one’s independence, Deep TMS offers a tool that directly addresses the brain’s dysfunction. It is not a cure. But it is a meaningful addition to what we can offer.” — Dr Nishit Sawal
To discuss whether Deep TMS may benefit your neurological condition, schedule a consultation with Dr Nishit Sawal at the Department of Neurology, Fortis Hospital Mohali. Please bring your current neurological assessments, medication list, and any imaging studies for a comprehensive evaluation.
About the Author
Dr Nishit Sawal is a Consultant Neurologist at Fortis Hospital, Mohali, with specialist expertise in movement disorders, stroke, and neuromodulation. He works jointly with the Department of Psychiatry to deliver Deep TMS for neurological indications including Parkinson’s disease and Alzheimer’s disease — the only such programme in the Chandigarh–Mohali–Panchkula tricity region. His clinical practice covers the full spectrum of neurological disorders, and he serves patients from across Punjab, Chandigarh, Haryana, Himachal Pradesh, and Jammu & Kashmir. This article was written and medically reviewed by Dr Sawal based on peer-reviewed clinical evidence and current 2026 research.
Categories
Clear allRelated Blogs
View all





FAQs
Can Deep TMS help my Parkinson’s medications work better?
The evidence suggests yes. The Torres study showed a 73% increase in daily ON time without any change in medication dosage, indicating that Deep TMS may potentiate the effect of levodopa. In some patients it may eventually allow dose adjustment, though this should only be done under neurological supervision.
How many sessions are needed for Parkinson’s disease?
Clinical trials used 12 to 14 sessions over 3 to 4 weeks, with benefits persisting for at least 30 days after treatment. With newer accelerated protocols emerging in 2026, treatment schedules may become shorter. Maintenance sessions may extend benefits further. Your neurologist will design a schedule for your situation.
Is Deep TMS appropriate for all stages of Alzheimer’s disease?
Available data suggests patients with moderate-to-severe disease may actually show the greatest improvement, and new trials are exploring its use in early cognitive decline. However, treatment decisions must be made case by case by your neurologist, considering the overall clinical picture and goals of care.
How is Deep TMS different from deep brain stimulation (DBS)?
DBS requires brain surgery to implant electrodes. Deep TMS is completely non-invasive — no surgery, no implants, no anaesthesia. It stimulates the brain from outside the skull using magnetic fields. For appropriate patients, this makes Deep TMS a lower-risk option, though DBS remains important for selected advanced Parkinson’s patients.
Are there risks specific to neurological patients?
In Parkinson’s patients with levodopa-induced dyskinesias, Deep TMS may temporarily induce mild dyskinesias — a sign that stimulation is enhancing dopaminergic activity. These are transient and not distressing. Standard TMS contraindications (metallic implants in the head, seizure history, cardiac pacemakers) apply, and every patient is screened before treatment.
Is Deep TMS available near me in Punjab or Chandigarh?
Fortis Hospital Mohali is the only centre in the Chandigarh–Mohali–Panchkula tricity region offering BrainsWay Deep TMS, serving patients from across Punjab, Haryana, Himachal Pradesh, and Jammu & Kashmir. The neurology programme is run by the Department of Neurology in coordination with Psychiatry.

Keep track of your appointments, get updates & more!

