






Hole in the Heart Narrow Valves and Blue Baby Symptoms A Pediatric Cardiologist Guide
By Dr. Rajat Gupta | Pediatric Cardiologist, Fortis Hospital Mohali
Specialist in fetal echocardiography, catheter-based (non-surgical) interventions for congenital heart defects, and pediatric cardiac intensive care. Reviewed for accuracy by the Department of Pediatric Cardiology, Fortis Hospital Mohali.
Every heartbeat matters—but when that heart belongs to a child, the stakes are infinitely higher. There is no sound more reassuring to a parent than the steady, rhythmic thumping of their child’s heart. Yet for thousands of families across India, that rhythm is interrupted by a reality they never anticipated: congenital heart disease (CHD).
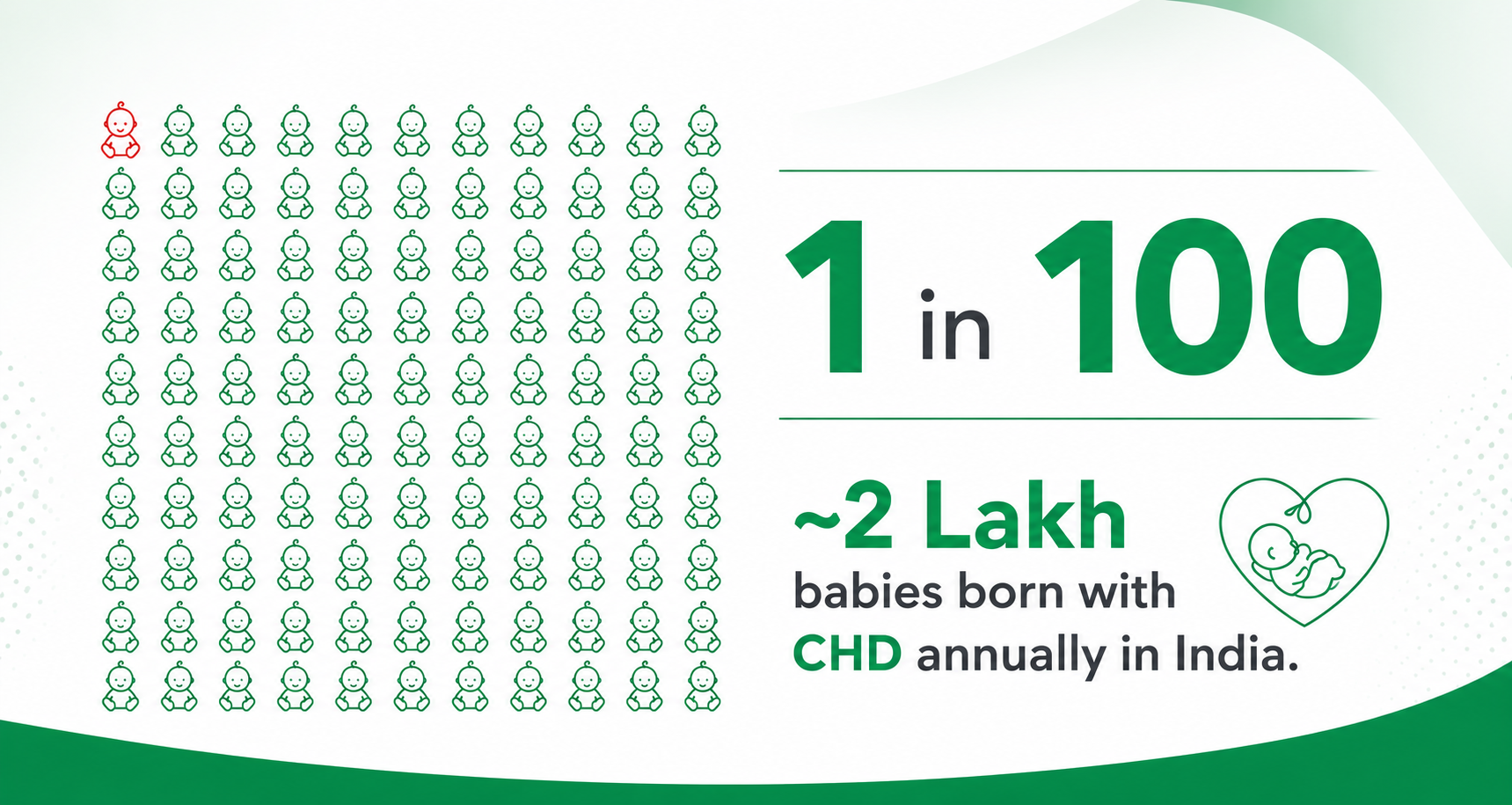
India carries one of the heaviest burdens of congenital heart disease in the world. With an estimated 1.8 to 2 lakh children born with heart defects every year, CHD is the most common birth defect in our country—nearly one in every hundred babies is born with some form of structural heart issue. Yet a tragically large number of these children go undiagnosed or untreated. This is not because the treatments do not exist, nor because the defects are always inoperable. It is primarily because families do not always know where to turn, and—more dangerously—they do not always recognise the early warning signs, or understand that the type of doctor they turn to matters immensely.
As a pediatric cardiologist practising at Fortis Hospital Mohali, my mission is to change that narrative: to bring awareness, precision, and hope to families navigating the complex world of childhood heart disease. This guide is written for parents who have typed worried questions into a search bar late at night—“Why is my baby breathing fast?”, “Why does my child get tired while playing?”, “What are the symptoms of a hole in the heart?”—and are looking for clear, trustworthy answers.
Warning Signs: When Your Child’s Symptoms May Point to a Heart Problem
Congenital heart defects often announce themselves through everyday feeding, breathing, and activity patterns—long before anyone mentions the word “heart.” Because a young child cannot describe what they feel, the symptoms show up in how they feed, breathe, grow, and play. The following signs are the ones parents most commonly search for, and the ones that should prompt an evaluation by a pediatric cardiologist.
Symptoms in babies and newborns
- Fast breathing in a baby — if your baby is breathing fast or breathing heavily even at rest, this can be an early sign of a heart defect straining the lungs.
- Baby gets tired while feeding, or sweating during feeding — feeding is a workout for an infant heart. A baby who tires quickly, pauses often, sweats on the forehead while feeding, or is not drinking milk properly may be signalling a problem.
- Poor weight gain in a baby or newborn — when the heart works overtime, calories are burned keeping the body going rather than helping the baby grow. Poor weight gain and a baby who seems weak and tired are important clues.
- Blue lips in a baby (blue baby syndrome) — a bluish tinge to the lips, tongue, or nail beds means oxygen-poor blood is reaching the body and needs urgent evaluation.
- A heart murmur in a newborn — an extra sound your pediatrician hears through the stethoscope. Many murmurs are harmless, but some are the first hint of a hole in the heart or a narrowed valve and deserve a specialist opinion.
- Fast heartbeat in a baby or newborn — a persistently racing heart, especially with fast breathing, should be checked.
Symptoms in older children
- “Why does my child get tired while playing?” — a child who cannot keep up with friends, gets breathless easily, or needs to stop and rest during play may have a heart that is working under strain.
- Frequent chest infections in a child — recurrent coughs, colds, and pneumonias can be linked to increased blood flow to the lungs from certain heart defects.
- Palpitations and breathlessness — an older child complaining of a fluttering or fast heartbeat along with shortness of breath should be evaluated.
- Breathlessness, chest pain while walking, or dizziness — these can point to a narrowed heart valve obstructing normal blood flow (discussed in detail below).
Note: A single symptom in isolation is rarely a diagnosis, and many children with these signs turn out to be perfectly healthy. But when these patterns persist—or occur together—they are the body’s way of asking for a closer look. Early evaluation is safe, painless, and can be life-changing.
A Pediatric Cardiologist Is Not Just a “Children’s Cardiologist”
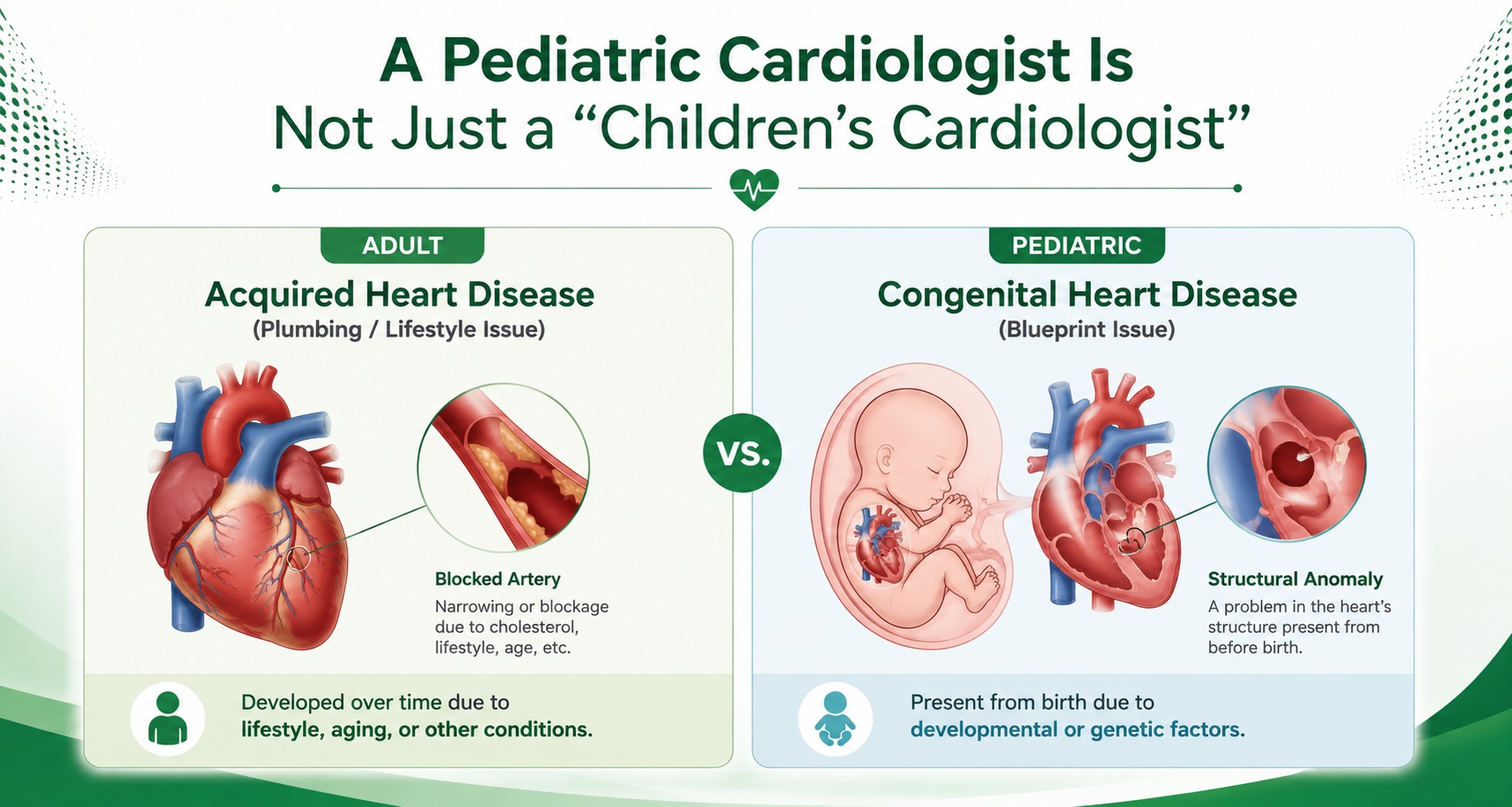
One of the most common—and potentially dangerous—misconceptions in medicine is the assumption that any cardiologist can treat a child. Families often seek out a respected adult cardiologist, believing that a heart is a heart, and a child is simply a smaller adult. In reality, nothing could be further from the truth.
Adult cardiologists are highly trained, vital specialists, but their expertise lies in conditions that develop over decades of living—coronary artery disease, hypertension, heart attacks, and age-related heart failure. These are “plumbing” problems that arise from lifestyle, ageing, and wear-and-tear. Congenital heart disease, by contrast, is a structural and developmental issue present from birth. It is a problem with the original blueprint.
The anatomy of a child with CHD is fundamentally different. The holes, the narrowed valves, the abnormal connections—these require a completely different physiological mindset. A child’s heart is not just small; it is still developing, and the hemodynamics (the way blood flows and pressures build) change dramatically in the first weeks and months of life.
A pediatric cardiologist undergoes years of specialised training in the structure and function of the developing heart—from fetal life through adolescence. We speak a different clinical language and use different tools. We understand that a medication dose calculated for a 3-kilogram newborn cannot simply be scaled down from an adult dose, and that a heart failing in an infant does not look like a heart failing in a seventy-year-old. Recognising these subtle, life-threatening differences is the cornerstone of pediatric cardiology, and it is why your child deserves a specialist.
Hole in the Heart Symptoms: Understanding ASD, VSD and PDA
When parents are told that their child has a “hole in the heart,” they often picture grueling open-heart surgery. The reality today is far less daunting. First, it helps to understand what these defects are and the symptoms they cause.
What is a hole in the heart? ASD, VSD and PDA explained
The heart has four chambers, with walls that separate the clean, oxygen-rich blood from the blue, oxygen-poor blood. A hole between the upper chambers is an Atrial Septal Defect (ASD); a hole between the lower chambers is a Ventricular Septal Defect (VSD). A Patent Ductus Arteriosus (PDA) is an abnormal vessel connection outside the heart that should naturally close at birth but sometimes remains open. All three allow blood to flow abnormally and can overload the lungs and heart.
Symptoms of an ASD (hole in the heart) in children
Many children with a small ASD have no symptoms and are picked up only when a doctor hears a heart murmur. When symptoms do appear, parents typically notice a child who gets tired or breathless easily while playing, suffers frequent chest infections, has palpitations and breathlessness, or—in babies—breathes fast, feeds poorly, sweats during feeding, and shows poor weight gain. A child who seems weak, tired, and is not gaining weight as expected deserves an echocardiogram to look for a hole in the heart.
PDA symptoms: why is my premature baby breathing heavily?
A Patent Ductus Arteriosus is especially common in premature babies. Parents and neonatal teams often notice a baby breathing fast or breathing heavily, sweating while feeding, tiring during feeds, feeding poorly, and gaining weight slowly, sometimes with a fast heartbeat and a heart murmur. In a premature baby who is breathing heavily and not feeding properly, a PDA is one of the important causes we actively look for and can treat effectively.
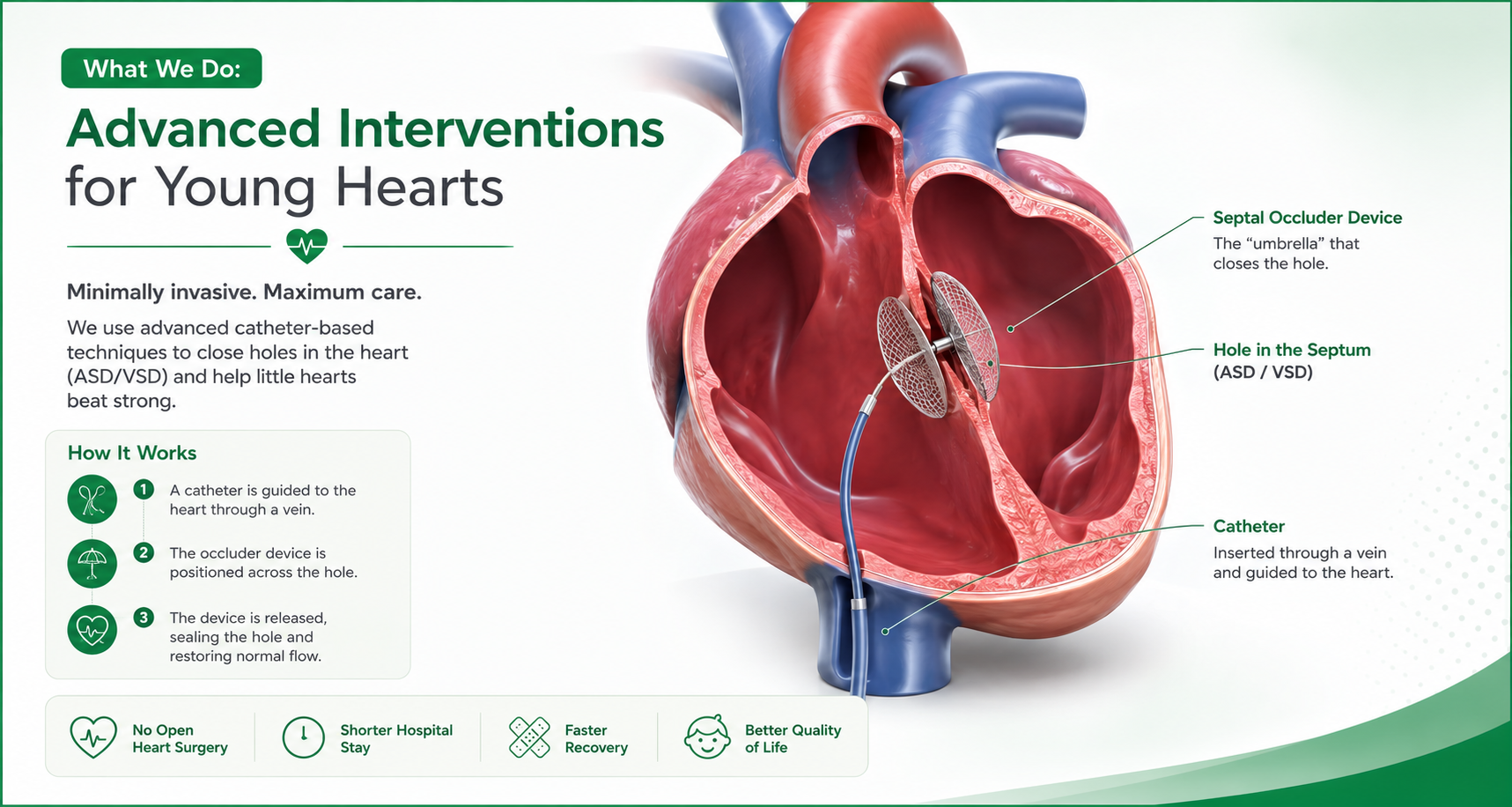
Non-surgical treatment: device closure of ASD, VSD and PDA
In the past, fixing these holes required opening the chest and patching them. Today, we thread a tiny, specialised catheter through a blood vessel in the groin, navigate it into the heart, and deploy a small, intricately designed metallic mesh device that unfolds like a tiny umbrella, plugging the hole from the inside. Within months, the heart’s own tissue grows over the device, making it a permanent part of the heart—no chest incision, no stopping the heart, and no long, painful recovery.
Narrow Heart Valve Symptoms and Treatment Without Surgery
Sometimes the “doors” of the heart—the valves—do not open properly, forcing the heart to strain as it pumps blood against a narrowed opening. This is called valve stenosis, and it commonly affects the pulmonary, aortic, or mitral valves. A child can be born with a narrow heart valve, or the narrowing can develop over time.
Symptoms of a narrowed heart valve
The symptoms of a narrow heart valve reflect a heart working against resistance: breathlessness due to the heart valve problem, chest pain while walking or on exertion, dizziness, a fast heartbeat with shortness of breath, and tiredness due to heart valve disease. In infants, valve stenosis can also cause fast breathing, poor feeding, and poor weight gain. If your child has these symptoms—or has been told they have pulmonary valve stenosis or aortic valve stenosis—the good news is that many narrowed valves can be treated without open surgery.
Can a heart valve blockage be treated without surgery? Balloon Valvotomy
Yes—for many patients, a narrowed valve can be opened without open-heart surgery through a procedure called Balloon Valvotomy (balloon dilatation). Using a catheter passed through a blood vessel, we guide a tiny, deflated balloon across the narrowed valve and inflate it to high pressure, gently tearing open the fused leaflets and restoring normal blood flow. The balloon is then deflated and removed. This is a well-established, non-surgical treatment for a narrowed heart valve—particularly effective for pulmonary valve stenosis and for aortic valve stenosis—offering an alternative to open surgery, a short hospital stay, and a rapid recovery with no chest scar.
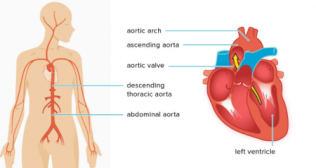
Stenting of Coarctation of the Aorta
The aorta is the body’s main highway, carrying blood from the heart to the rest of the body. In some children this highway has a severe narrowing (coarctation), forcing the heart to pump against intense resistance. Today we can treat this by placing a small metallic stent through a catheter, expanding it at the site of the narrowing to prop the artery open like a scaffold and restore normal blood flow.
These catheter-based procedures are performed in our fully equipped, state-of-the-art cath lab. The most reassuring part? They usually require just a short hospital stay—often a day or two—and children are back home, running and playing, with only a tiny bandage on the groin to show for it. There are no massive chest scars, and the psychological trauma of major surgery is avoided.
Fetal Cardiology: Diagnosing a Heart Defect Before Birth

One of the most powerful tools we have is fetal echocardiography—a specialised, detailed ultrasound of the unborn baby’s heart, performed as early as 18–22 weeks of pregnancy. While a routine obstetric ultrasound checks growth and basic anatomy, a fetal echo looks specifically at the intricate architecture of the heart: the chambers, the valves, the major vessels, and the blood-flow dynamics.
Detecting a heart defect before birth transforms the trajectory of care. It means families can plan, rather than being blindsided at birth by a baby turning blue or struggling to breathe. It means our genetic counsellors and psychologists can prepare the family, and our neonatal and cardiac teams can be ready the moment the baby takes its first breath—orchestrating the delivery so the baby is immediately stabilised and transferred to the cardiac ICU. This prevents the severe organ damage that can occur when a heart defect goes undiagnosed in the crucial first hours of life. In many cases, this early warning is the difference between life and death.
When Surgery Is Needed: We’re Ready
While non-surgical interventions have changed the landscape of pediatric cardiology, they cannot fix everything. For highly complex defects—such as Tetralogy of Fallot, Transposition of the Great Arteries, or severe underdevelopment of a heart chamber—open-heart surgery remains the gold standard. When surgery is required, families at Fortis Mohali are surrounded by a comprehensive, integrated team offering a full spectrum of congenital heart surgeries, backed by a dedicated Pediatric Cardiac ICU.
A Pediatric Cardiac ICU is not a corner of an adult ICU with a smaller bed. It is a specialised space designed entirely for children—from ventilators built for tiny lungs to micro-drip infusion pumps that deliver medications in fractions of a milliliter—staffed by intensivists, nurses, and technicians who understand that a child’s recovery is not simply a smaller version of an adult’s. Children have different fluid tolerances, different responses to pain, and different emotional needs. Our team is trained to treat the whole child: not just the heart, but the frightened toddler who needs their mother’s hand and the anxious parents who need clear, compassionate communication.
A Heart Fixed in Time Changes a Life Forever

The tragedy of congenital heart disease in India is not just that children are born with it, but that so many live with it undiagnosed. Children with untreated defects often live on the sidelines—unable to keep up with friends on the playground, suffering frequent lung infections, struggling to gain weight, and tiring easily. Over time, the unrelenting strain can cause irreversible damage to the heart muscle and the blood vessels of the lungs, reaching a point where even a successful repair becomes impossible.
But here is the hope: most children treated for congenital heart disease go on to lead full, active, healthy lives. A heart fixed in time allows a child to run without losing breath, to grow to their full potential, and to live without the shadow of heart failure. The window for treatment is often time-sensitive—the earlier we intervene, the better the long-term outcomes for the child’s brain, body, and emotional development.
Your Child’s Heart Deserves a Specialist
If you have been told that your child—or your unborn baby—has a heart problem, or if you recognise these warning signs, please do not adopt a “wait and see” approach and do not assume they will simply outgrow it. Early evaluation and timely intervention can make all the difference. At Fortis Hospital Mohali, we are here to ensure every heartbeat counts.
Categories
Clear allMeet the doctor

- Cardiac Sciences | Paediatric CTVS (Cardiothoracic and Vascular Surgery)
-
 16 Years
16 Years
-
 550
550
Related Blogs
View all







FAQs
Why does my child get tired while playing or get breathless easily?
A child who cannot keep up with friends, gets breathless easily, or needs frequent rest during play may have a heart working under strain—often from a hole in the heart (ASD/VSD) or a narrowed valve. Persistent exercise intolerance in a child should be evaluated with a simple, painless echocardiogram.
Why is my baby breathing fast or breathing heavily?
Fast or heavy breathing at rest can be an early sign of a heart defect overloading the lungs, such as a large PDA, VSD, or ASD. In premature babies especially, a Patent Ductus Arteriosus (PDA) is a common and treatable cause. Rapid breathing that persists deserves prompt assessment.
Why is my baby not gaining weight or feeding poorly?
When a baby’s heart works overtime, calories are spent keeping the body going rather than helping the baby grow. Poor weight gain, tiring while feeding, sweating during feeds, and not drinking milk properly are classic signs of an underlying heart defect and should be checked by a paediatric cardiologist.
Why does my baby sweat during feeding?
Sweating on the forehead during feeding—often with pauses, fast breathing, and tiredness—is a well-recognised sign that feeding is straining the heart. It is one of the most useful early clues to a congenital heart defect in infants.
What are the symptoms of a hole in the heart?
Common symptoms include tiring or breathlessness while playing, frequent chest infections, palpitations, fast breathing in babies, poor feeding and poor weight gain, and sometimes a heart murmur heard by the doctor. Many small holes cause no symptoms and are found incidentally.
Why are my baby’s lips blue (blue baby syndrome)?
A bluish tinge to the lips, tongue, or nail beds—sometimes called blue baby syndrome—means oxygen-poor blood is reaching the body. This is a warning sign of certain congenital heart defects and needs urgent evaluation by a specialist.
Is a heart murmur in a newborn dangerous?
Many newborn murmurs are innocent and harmless. However, some are the first sign of a hole in the heart or a narrowed valve. Because it is impossible to tell them apart by listening alone, a murmur in a newborn is best evaluated with an echocardiogram by a pediatric cardiologist.
Can a heart valve blockage be treated without surgery?
Yes. Many narrowed valves—particularly pulmonary and aortic valve stenosis—can be opened without open-heart surgery using Balloon Valvotomy, a catheter-based procedure that inflates a small balloon across the valve to restore normal blood flow. It offers a short hospital stay and rapid recovery with no chest scar.

Keep track of your appointments, get updates & more!

