





National Heart Valve Disease Awareness Day: Small Valves, Serious Warnings
Four tiny structures regulate blood flow through the heart with remarkable precision, opening and closing billions of times across a lifetime. When these valves malfunction, subtle symptoms often emerge years before life-threatening complications develop. National Heart Valve Disease Awareness Day emphasises recognising warning signs that many dismiss as normal ageing or general fatigue.
Heart valve problems develop gradually through congenital abnormalities, degenerative changes, infections, or rheumatic fever sequelae. Early detection dramatically improves outcomes by enabling intervention before irreversible damage occurs. Understanding heart valve disease awareness alongside identifying valve disease early signs helps individuals seek evaluation when symptoms signal developing problems.
Understanding How Valve Dysfunction Develops Over Time
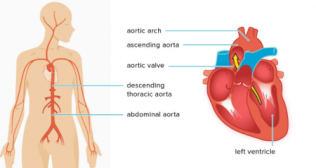
Heart valves consist of thin tissue flaps that open with each heartbeat, allowing blood to flow forward, then close, preventing backward leakage. Stenosis occurs when valve leaflets thicken or fuse together, narrowing the opening. Regurgitation develops when leaflets fail to close completely, allowing blood to leak backwards. Some patients experience both stenosis and regurgitation simultaneously.
Degenerative changes represent the most common cause, with calcium deposits gradually stiffening valve leaflets. Bicuspid aortic valve; a congenital condition where the valve forms with two leaflets instead of three, accelerates degeneration. Rheumatic heart disease damages valves through autoimmune inflammation following streptococcal infections. Endocarditis creates valve damage when bacteria colonise surfaces, destroying tissue through infection.
Recognising Subtle Symptoms Before Obvious Cardiac Distress
Valve disease early signs often masquerade as general deconditioning rather than cardiac pathology. Fatigue develops insidiously as reduced cardiac output fails to meet oxygen demands during routine activities. Breathlessness climbing stairs or walking moderate distances suggests inadequate circulation. Palpitations occur when the heart compensates for inefficient pumping through increased rate or irregular rhythms.
Swollen ankles signal fluid retention when valve dysfunction impairs cardiac efficiency. Dizziness or lightheadedness accompanies severe valve narrowing that restricts brain blood flow. Chest discomfort emerges when increased cardiac workload exceeds oxygen supply. These symptoms progress gradually, allowing patients to unconsciously adjust activity whilst disease worsens.
Why Heart Valve Disorder Symptoms Remain Underdiagnosed
Many people attribute progressive fatigue to advancing age or poor fitness without considering cardiac causes. Breathlessness develops so gradually that individuals adapt by reducing activities. Healthcare providers sometimes miss valve disease during examinations when murmurs remain subtle. Standard electrocardiograms detect rhythm abnormalities but may appear normal despite dysfunction.
The compensatory mechanisms maintaining circulation initially mask disease severity. The heart enlarges to pump more forcefully, temporarily preserving function despite worsening pathology. This compensation eventually fails when demands exceed capacity to adapt. Symptoms then accelerate rapidly after years of silent progression.
Advanced Diagnostic Approaches Reveal Structural Abnormalities
Echocardiography provides detailed visualisation of valve structure and function through non-invasive ultrasound imaging. This technique measures how much blood leaks backward or estimates valve opening size precisely. Doppler studies assess blood flow patterns and velocities through affected valves quantitatively. These measurements guide treatment decisions by objectively documenting disease severity beyond subjective symptoms alone.
Cardiac catheterisation offers invasive assessment when echocardiography provides insufficient information for treatment planning. This procedure measures pressures within heart chambers whilst directly visualising valve function through contrast injection. Exercise stress testing reveals symptoms or blood pressure abnormalities that emerge only during exertion. Cardiac sciences programmes integrate these diagnostic modalities to characterise valve disease comprehensively before recommending intervention strategies.
Treatment Options Range From Monitoring to Surgical Replacement
Mild valve disease requires only periodic monitoring through serial echocardiograms tracking progression rates. Medications manage symptoms or address underlying conditions contributing to valve dysfunction. Antibiotics prevent endocarditis in high-risk patients undergoing dental or surgical procedures. These conservative approaches suit individuals with minimal symptoms and preserved cardiac function.
Moderate to severe disease necessitates valve repair or replacement restoring normal blood flow patterns. Surgical repair reconstructs damaged valves whilst preserving native tissue when anatomically feasible. Replacement substitutes diseased valves with mechanical or biological prostheses when repair proves impossible. Facilities offering comprehensive cardiac sciences services like Fortis Healthcare, Gurgaon provide both open-heart surgery and minimally invasive approaches tailored to individual patient circumstances. Advanced centres integrate surgical expertise with sophisticated imaging and anaesthetic capabilities essential for optimal outcomes.
Transcatheter Procedures Expand Treatment Options
Transcatheter aortic valve replacement delivers prosthetic valves through catheters inserted via peripheral arteries, avoiding open-heart surgery entirely. This approach benefits elderly patients or those with medical conditions increasing surgical risks substantially. Mitral valve clips repair certain types of regurgitation through catheter-based techniques. These minimally invasive interventions reduce recovery times whilst expanding treatment accessibility.
Patient selection requires careful evaluation balancing procedural risks against expected benefits. Frail individuals who couldn't tolerate traditional surgery sometimes achieve remarkable improvements through transcatheter approaches. Anatomical considerations determine which patients qualify for catheter-based versus surgical interventions. Multidisciplinary heart teams review complex cases collaboratively to recommend optimal treatment strategies.
Building Heart Valve Disease Awareness Through Community Education
Screening programmes identify asymptomatic valve disease in at-risk populations before symptoms develop. Individuals with heart murmurs detected during routine examinations warrant echocardiographic evaluation. Those with rheumatic fever history require ongoing surveillance despite feeling completely well. Family screening benefits relatives of patients with bicuspid aortic valves or other genetic valve abnormalities.
Public education emphasises that heart valve disorder symptoms deserve medical attention rather than dismissal as normal ageing. Awareness campaigns teach people to recognise progressive fatigue, breathlessness, or swelling as potential cardiac warnings. Early detection enables intervention before irreversible heart damage develops. These educational efforts complement diagnostic services by encouraging timely consultation when symptoms emerge.
Managing Life After Valve Intervention
Anticoagulation therapy prevents blood clots in patients receiving mechanical valve replacements throughout their remaining lifetime. Regular monitoring ensures anticoagulation levels remain therapeutic without causing bleeding complications. Biological valves eventually deteriorate, sometimes requiring replacement after 10-20 years. Patients must weigh durability against anticoagulation requirements when choosing prosthesis types.
Endocarditis prevention remains crucial following valve repair or replacement procedures. Prophylactic antibiotics before dental work or certain medical procedures reduce infection risks. Patients learn to recognise fever or new symptoms suggesting possible valve infection requiring urgent evaluation. Regular cardiology follow-up tracks valve function whilst screening for developing complications.
Exercise and Activity Modifications Support Cardiac Health
Most patients resume normal activities following successful valve intervention after appropriate recovery periods. Competitive athletics may require restriction depending on residual valve dysfunction or prosthesis type. Regular moderate exercise improves cardiovascular fitness whilst supporting healthy weight maintenance. Individual recommendations consider specific valve pathology, intervention type, and overall cardiac function.
Pregnancy planning requires specialised counselling for women with valve disease considering childbearing. Some valve conditions or prosthesis types increase pregnancy risks substantially. Medication adjustments may become necessary to protect both mother and developing foetus. Coordinated care between cardiologists and obstetricians optimises outcomes when pregnancy proceeds.
Understanding Genetic Implications for Family Members
Similar symptoms appearing in multiple family members suggest possible genetic valve conditions warranting relative screening. Bicuspid aortic valve demonstrates familial clustering, with first-degree relatives facing increased risks. Connective tissue disorders like Marfan syndrome cause valve problems requiring family evaluation. Genetic counselling helps families understand inheritance patterns whilst guiding screening recommendations.
Early detection in asymptomatic relatives enables monitoring before symptoms develop or damage accumulates. Some individuals benefit from prophylactic interventions preventing complications. Family screening programmes identify at-risk individuals who might otherwise remain undiagnosed until advanced disease. These proactive approaches improve outcomes through early intervention opportunities.
Categories
Clear allRelated Blogs
View all








Keep track of your appointments, get updates & more!

