






Obesity Control Options in 2026: From Apps to Metabolic & Bariatric Surgery
Obesity (severe weight gain) affects more than 135 million Indians today, including a rapidly growing number of individuals across Punjab. For decades, we treated it as a character flaw, a failure of discipline. That framing was wrong, and it prevented millions from getting effective treatment. The medical community now recognizes obesity as a chronic, relapsing metabolic disease, one that requires the same structured approach we apply to diabetes or hypertension.
The good news: effective treatments exist across a spectrum of intensity. The challenge: knowing which option fits your specific situation. A 28-year-old with BMI 29 and no health complications needs a completely different approach than a 45-year-old with BMI 42, Type 2 diabetes, and sleep apnea.
This guide walks through every major obesity control option available in India, from digital health apps to bariatric surgery (commonly known as weight loss surgery). Each comes with genuine benefits and real limitations. Understanding both is essential before choosing your path forward.
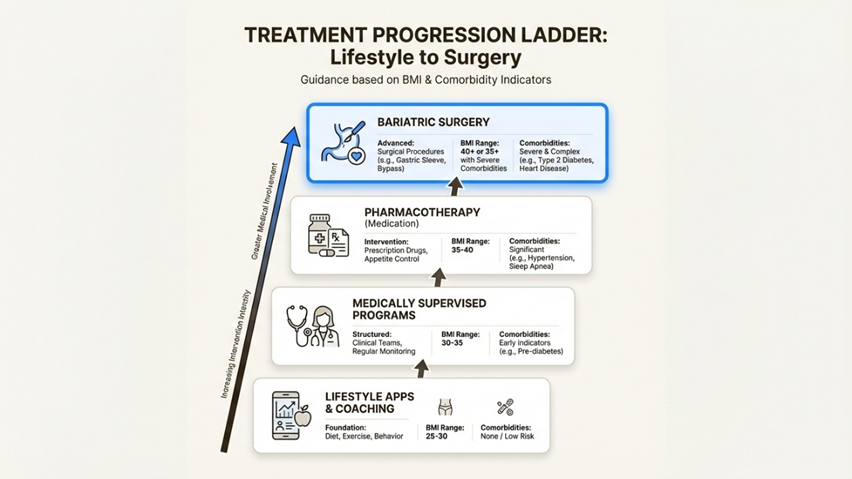
Each step up represents more intensive intervention as BMI and comorbidities increase.
Understanding obesity as a chronic disease
Before exploring treatments, two mindset shifts matter. First, obesity is not about willpower. Research consistently shows that genetic, hormonal, environmental, and psychological factors drive weight gain and make weight loss difficult to sustain. Second, the goal is not just a number on the scale. Effective treatment targets blood sugar control, blood pressure reduction, sleep apnea resolution, fatty liver improvement, joint pain relief, fertility restoration, and overall quality of life.
Treatment selection follows what clinicians call the "Ladder of Intervention." You start with the least invasive options and escalate based on severity, response, and personal readiness. Someone with mild obesity and no metabolic complications might achieve lasting results with lifestyle modification and digital tools. Someone with severe obesity and multiple comorbidities often needs surgery (a fat loss operation) to achieve meaningful, durable improvement.
Before choosing any treatment, your care team should conduct a baseline assessment covering:
- BMI and waist circumference measurement to establish severity
- Comorbidity evaluation for conditions like Type 2 diabetes, hypertension, sleep apnea, and PCOS
- Lifestyle review including diet history, physical activity levels, sleep quality, stress, alcohol consumption, and smoking status
- Screening for secondary causes such as hypothyroidism, PCOS, depression, or binge eating disorder
- Lab work and cardiovascular risk profiling to understand overall metabolic health
This assessment guides which rung of the treatment ladder makes sense for you. Skipping this step often leads to mismatched expectations and poor outcomes.
Digital health and lifestyle support with HealthifyMe
For people with mild to moderate obesity (BMI 25-32) without significant comorbidities, digital health platforms offer an accessible starting point. HealthifyMe is Asia's largest health and fitness app, with over 40 million users globally and a comprehensive database of more than 100,000 foods focused on Indian cuisines.
The platform's core feature is Ria, an AI coach available 24/7 for personalized meal planning, recipe suggestions, and accountability support. The SNAP feature uses AI-powered image recognition to log meals instantly, reducing the friction of manual food tracking. Premium tiers add human coaching from certified nutritionists and fitness trainers.
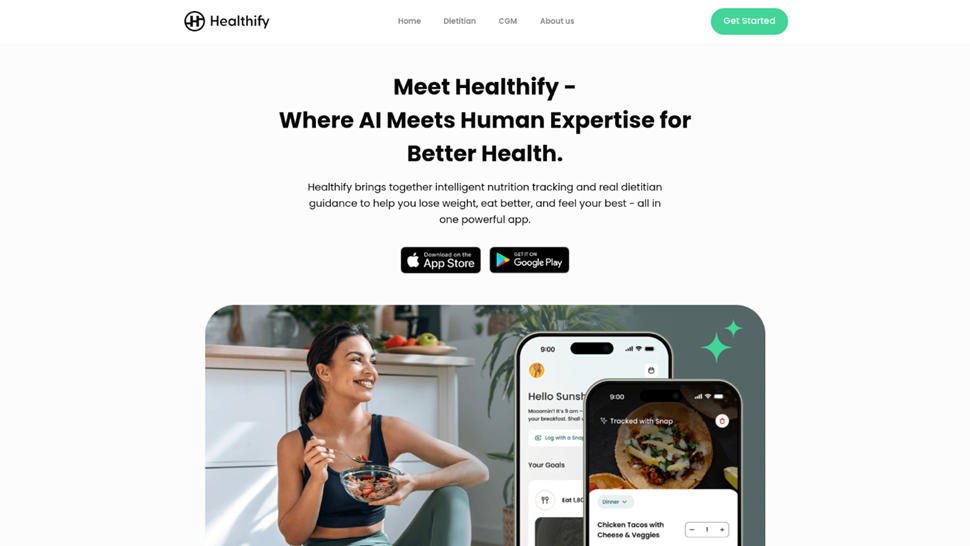
What distinguishes HealthifyMe in the Indian context is its integration with clinical care. Fortis Hospital, Mohali has partnered with HealthifyMe to bridge digital coaching with professional obesity care, creating a pathway from app-based habit formation to clinical intervention when needed.
Benefits
HealthifyMe works well as an entry point because it builds awareness around food choices and eating patterns. The 24/7 AI availability removes scheduling barriers. Company data claims users see an average weight loss of 1.2 kg per week, with 80% reporting improvement in obesity-related conditions and greater than 15% reduction in HbA1c levels for diabetic users. At approximately Rs 3,400-4,000/month for premium plans (or Rs 41,250-48,180/year for annual subscriptions), it is significantly more affordable than procedural interventions.
Considerations
Digital tools require consistent self-motivation. Results depend heavily on honest food logging, and many users underreport intake. For severe obesity (BMI 40+), standalone app-based approaches rarely produce sufficient weight loss. Trustpilot reviews reveal a gap between app functionality and premium service delivery, with some users reporting coach availability issues, generic diet plans, and difficulty obtaining refunds. The platform works best as a maintenance tool after more intensive intervention, not as primary treatment for significant obesity.
- Best for: BMI 25-32 without significant comorbidities, or as a long-term maintenance tool following other treatments.
Pharmacotherapy: GLP-1 agonists for appetite regulation
GLP-1 receptor agonists (widely known by patients as weight loss injections or appetite suppressants) represent a genuine advancement in obesity pharmacotherapy. These injectable medications work through multiple pathways: activating receptors in the hypothalamus to reduce hunger signals, slowing gastric emptying to prolong satiety, and improving blood sugar control. Originally developed for Type 2 diabetes, they are now approved specifically for weight loss.
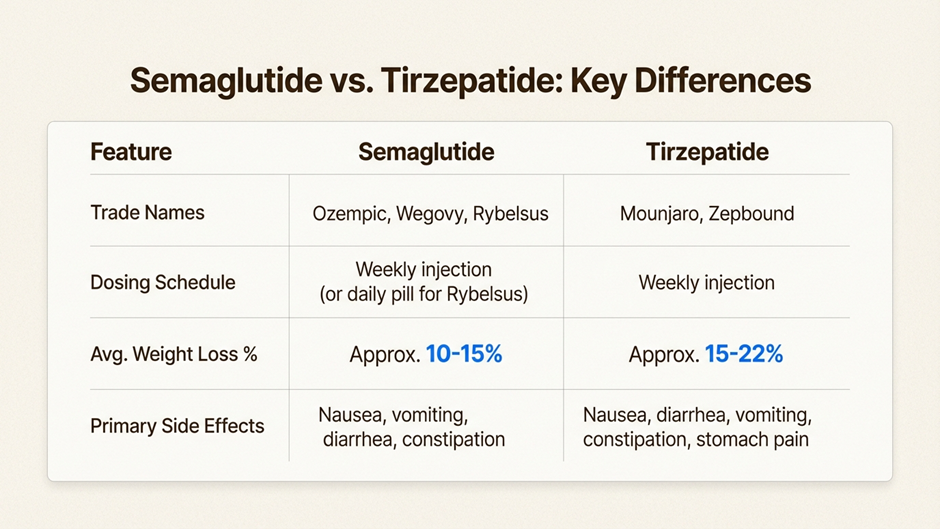
The two primary medications are:
- Semaglutide (brand names: Ozempic for diabetes, Wegovy for weight loss)
- Tirzepatide (brand names: Mounjaro for diabetes, Zepbound for weight loss)
Clinical trials show 15-16% total body weight loss with semaglutide and 14-18% with tirzepatide over 6-12 months. Both achieve significantly more weight loss than lifestyle modification alone (typically 3-5%) but less than bariatric surgery.
Benefits
GLP-1 medications offer a non-surgical, reversible option with genuine metabolic benefits beyond weight loss. Improvements in blood sugar control and cardiovascular risk markers are well-documented. For patients unable or unwilling to undergo surgery, these medications can serve as standalone treatment. For those considering surgery, they can serve as a bridge, helping reduce surgical risk through pre-operative weight loss.
Considerations
The most common side effects are gastrointestinal: nausea, vomiting, and diarrhea. These typically improve with slow dose titration but cause some patients to discontinue treatment. "Ozempic face," facial volume loss from rapid weight reduction, is a recognized aesthetic concern.
The more significant issue is weight regain. Clinical data indicates 15-20% of lost weight returns upon medication discontinuation. This creates a practical decision: commit to lifelong therapy or accept weight regain. At approximately Rs 75,000-1,50,000/month in India (or $1,000-1,500/month in the US) without insurance, long-term costs are substantial.
Absolute contraindications include personal or family history of medullary thyroid cancer (MTC) and Multiple Endocrine Neoplasia type 2 (MEN2). Pancreatitis risk and increased gallbladder disease are additional warnings requiring monitoring.
- Best for: BMI 30-40 with metabolic comorbidities, patients not ready for procedural intervention, or as a bridge toward surgery.
Swallowable devices: The Allurion gastric balloon
The Allurion Balloon (often searched for as a stomach balloon for weight loss or a swallowable weight loss pill) represents a unique category in obesity treatment: a gastric space-occupying device that requires no surgery, endoscopy, or anesthesia for placement or removal. The device is swallowed as a capsule, inflated with 550ml of sterile water inside the stomach, and remains for approximately 16 weeks before a time-release valve opens and it passes naturally through the digestive system.
The placement procedure takes 15-20 minutes in a clinic setting. The patient swallows the capsule (attached to a thin catheter), an X-ray confirms positioning, the balloon is filled, and the catheter is removed. Clinical data from nearly 20,000 patients shows 99.9% successfully swallow the capsule.
Benefits
The Allurion Balloon's primary advantage is its truly non-invasive nature. No operating room, no anesthesia, no endoscopy. Same-day discharge is standard. Clinical results show 10-15% total body weight loss over the 16-week period, with company data claiming 96% of weight loss maintained at 12 months when combined with their behavioral support program.
For patients in Chandigarh seeking a non-surgical jumpstart, the device is available through certified centers with integrated coaching support including the Allurion Connected Scale and mobile app with AI-powered Coach Iris.
Considerations
The balloon is temporary by design. After 16 weeks, it deflates and passes naturally. If eating behaviors do not change during this window, weight regain is common. Initial discomfort (nausea, fullness) for 24-48 hours post-placement is typical and can be significant for some patients.
The most important limitation for some readers: the Allurion Balloon is not FDA approved in the United States. It is available in Europe, Latin America, and Asia (including India), but patients seeking treatment in the US cannot access this specific device.
Cost in India ranges from Rs 3-5 lakhs (approximately $3,600-6,000 USD equivalent), typically not covered by insurance.
- Best for: BMI 27-35 seeking a non-surgical jumpstart; patients not ready for more invasive procedures; bridge to more definitive treatment.
Endoscopic procedures: ESG as the middle ground
Endoscopic Sleeve Gastroplasty (ESG) — often called non-surgical stomach reduction — fills the gap between temporary devices and permanent surgery. The procedure involves passing an endoscope through the mouth (no external incisions) and placing sutures inside the stomach to reduce its volume by approximately 70%. The result is a sleeve-like stomach structure similar to surgical sleeve gastrectomy, but without removing any tissue.
The American Society for Metabolic and Bariatric Surgery (ASMBS) officially endorsed ESG in 2024 as an approved procedure for obesity treatment, with international recognition from IFSO, NICE (UK), and multiple national surgical societies. The MERIT randomized trial reported 13.6% mean total body weight loss at 12 months, with peer-reviewed series typically showing 15-17.5% loss at 12-24 months.
Benefits
ESG offers several advantages over traditional surgery. Recovery is faster (2-3 days versus 1-2 weeks), there are no external incisions or visible scars, and the procedure carries lower perioperative risk. For patients who fail medical and behavioral management but are not ready for (or are poor candidates for) surgery, ESG provides a meaningful procedural option.
The Gastroenterology departments at Fortis hospitals work within multidisciplinary obesity programs to offer ESG as part of the treatment continuum in the Tricity region, with nutritional, behavioral, and medical support comparable to bariatric surgery programs.
Considerations
ESG weight loss is moderate compared to surgery. While 13-17% total body weight loss is clinically meaningful, bariatric surgery achieves 60-80% excess weight loss with stronger durability.
Suture durability is an evolving concern. Some evidence suggests sutures may loosen over 3-5 years, potentially reducing long-term effectiveness. Ten-year outcome data is still being collected. Complication rates are low (1.5-2.3%) but include bleeding and (rarely) perforation. Cost in India is approximately Rs 8-12 lakhs, generally not covered by standard insurance. Additionally, prior ESG can complicate future bariatric surgery if needed, as sutures can distort anatomy and create technical challenges.
- Best for: BMI 30-40, failed medical/behavioral management, not ready or higher-risk for surgery, seeking middle ground between medications and surgery.
Bariatric Surgery: The Gold Standard for Moderate - Severe Obesity
For patients with BMI 30+ and obesity-related health conditions (or BMI 35+ regardless of comorbidities), Bariatric Surgery (permanent weight loss surgery) remains the most effective and durable treatment available. The evidence base spans decades, with well-documented outcomes that no other intervention matches.
Surgery works through multiple mechanisms beyond simple stomach restriction: hormonal changes (particularly reduced ghrelin production), metabolic reset, altered gut hormone signaling, and microbiome shifts. These physiological changes explain why surgical weight loss is more durable and sustained than that achieved through diet alone.
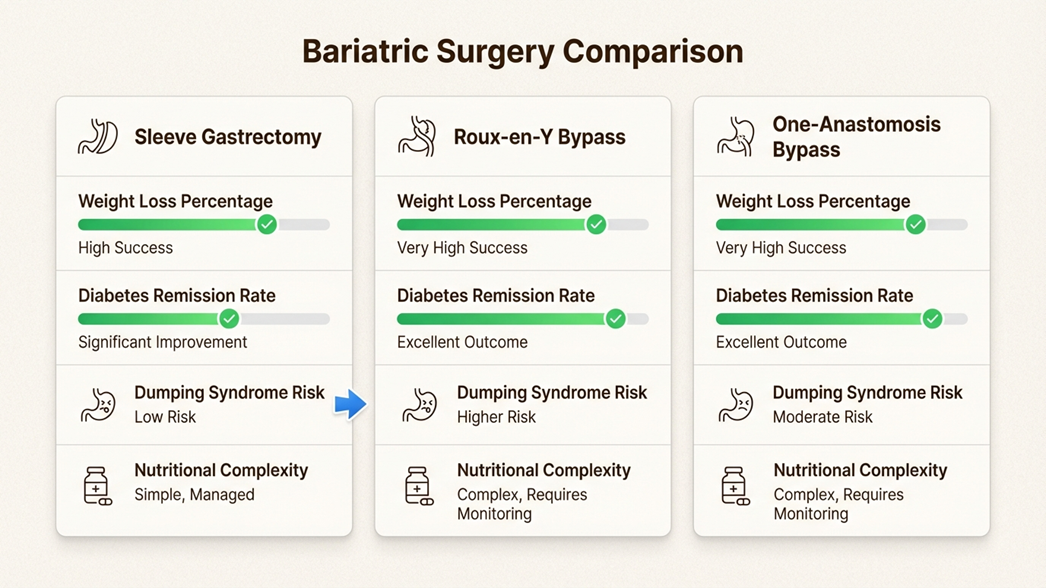
Types of bariatric procedures
- Sleeve gastrectomy involves removing approximately 80% of the stomach, leaving a tube-like structure. Weight loss averages 60-80% of excess weight. The procedure reduces ghrelin production, directly lowering appetite. It also results in a faster gastric emptying which increases the endogenous GLP-1 levels. There is no intestinal bypass which means there are no nutrient absorption issues.
- Roux-en-Y gastric bypass (RYGB) creates a small stomach pouch and reroutes the small intestine to connect directly to it. This combines restriction with malabsorption for powerful metabolic effects. It achieves the highest diabetes remission rates (50-85% of patients) and strongest cardiovascular benefits.
- One-anastomosis gastric bypass (OAGB/Mini-bypass) is a hybrid approach with simpler anatomy and single anastomosis. It also achieves high remission rates of diabetes mellitus and is a strong metabolic procedure. Therefore, it is increasingly being used as an alternative.
Benefits: Why surgery is the gold standard
The efficacy numbers make the case clearly:
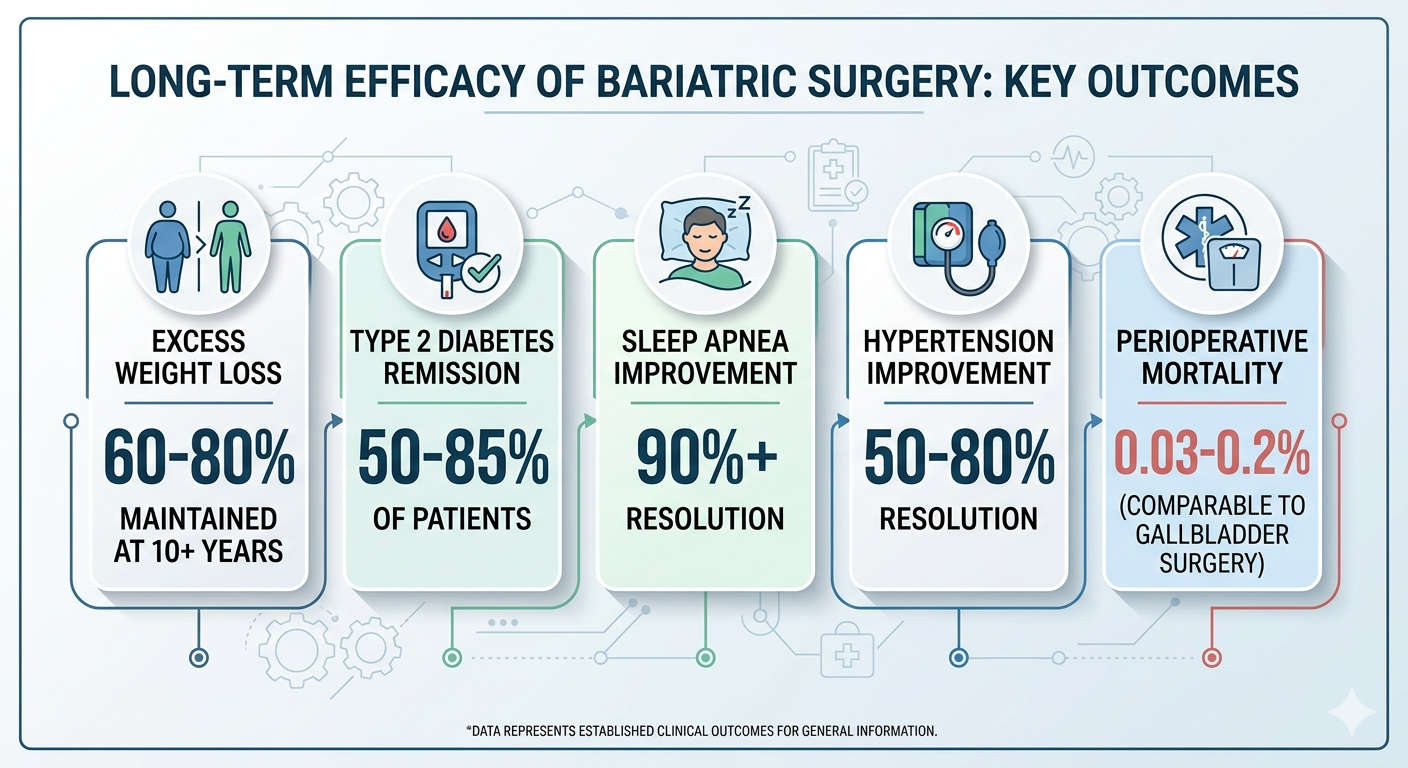
Beyond weight loss, surgery produces what clinicians call "disease reversal." Many patients reduce or eliminate diabetes medications. Majority of the patients are able to stop the use of insulin and oral drugs for diabetes as early as second day after surgery. CPAP machines for sleep apnea become unnecessary. Blood pressure normalizes. Joint pain decreases as mechanical load reduces. Quality of life improvements are substantial and well-documented.
For patients considering surgery, the Metabolic & Bariatric Surgery program at Fortis offers a multidisciplinary approach: Bariatric Surgeons working alongside endocrinologists, dietitians, and psychologists.
Considerations: What to consider
Bariatric surgery is major surgery. With advanced techniques, the risk of bleeding, infection, and anastomotic leak (where surgical connections fail) is very rare (<1%) and similar to other common surgeries like surgery for gall bladder stones and hernia surgeries. Careful surgeon selection and high-volume centers further minimize these risks.
Patients require:
- Lifelong vitamin supplementation: Vit B12 and Iron, calcium, folate, and vitamin D (specially if you are undergoing a bypass surgery)
- Dietary changes: High protein intake (1.2-1.5g/kg body weight), small portions. This comes naturally following the surgery due to ‘beneficial’ hormonal changes.
- Regular medical follow-up: The patients are called for follow at 1 week, 1 month, 3 months, 6 months and then every year following the surgery.
Will I regain weight? What are the chances that I will require of a second surgery?
The myth that everyone regains weight after bariatric surgery is false. If we look at global figures, 80% of patients do not regain weight over long term (>10 years). Around 15% patients regain some amount of weight but are still below the pre-surgery weight. Only 5% of patients regain weight to pre-surgery levels. The common causes of weight regain include irregular follow up, not following dietary advice and decreased physical activity. Regular follow up with the doctors has shown to reduce the chances of weight regain. Only few patients (<5% in our series) require second bariatric surgery.
Are there any large cuts during surgery?
No, there are no large incisions on your abdomen. The surgery is performed laparoscopically through 4-5 small cuts (each less than or equal to 1.5 cm). The recovery from surgery is quite rapid and the patient is mobilised 6 hours after surgery. The patients are usually discharged on second day after surgery. There is no requirement of bed rest following surgery.
How can I prevent development of loose skin?
Loose skin folds develop due to rapid loss. Skin being an elastic tissue has a tendency to return in shape with weight loss. Adequate protein intake, hydration and exercise are the key factors, which prevent development of loose skin following surgery. Loose skin usually develops in the stomach, arms, and thigh areas. If you choose, you may have plastic surgery to correct the loose skin. This procedure should be done only after you have lost all your weight, and usually is performed about 2-3 years after the initial bariatric surgery when the weight is at a plateau. In our experience, only a few patients have required this surgery.
What is the cause of hair fall following and is it permanent?
Some patients might experience hair fall following surgery. However, it is a temporary phase and all the hair will return. The common causes of hair fall include diet low in protein, iron, biotin and zinc. The hair fall can be reversed with supplementations of these nutrients. Hair fall is phasic (known as telogen effluvium in medical terms). It will end ultimately when the phase of hair growth (anagen effluvium) sets in.
Candidacy criteria
BMI Category
Recommendation
BMI 35+
Clear indication for surgery
BMI 30-34.9 with comorbidities
Strong indication (T2DM, hypertension, sleep apnea)
BMI 30-35 with uncontrolled diabetes
Clear indication (Surgery outperforms any sort of medical management)
Choosing the right treatment: A decision framework
Selecting among obesity control options requires matching treatment intensity to clinical need. The framework below provides guidance, though individual circumstances always require personalized medical evaluation.
Treatment recommendations by BMI category
- BMI 25-30 (Overweight): Start with structured lifestyle modification and digital tools like HealthifyMe. Consider pharmacotherapy if metabolic comorbidities are present. Surgery is rarely indicated unless exceptional circumstances exist.
- BMI 30-35 (Class I Obesity): Combine structured lifestyle with pharmacotherapy (GLP-1 agonists). Consider endoscopic procedures (ESG, Allurion) if medications are ineffective or contraindicated. Surgery becomes indicated if Type 2 Diabetes remains uncontrolled despite medical management.
- BMI 35-40 (Class II Obesity): Seek early consultation with a bariatric surgeon. GLP-1 medications or endoscopic procedures may serve as bridges to surgery. Surgery is strongly indicated when comorbidities are present.
- BMI 40+ (Class III/Severe Obesity): Bariatric surgery is the first-line treatment recommendation. Lifestyle modifications and medications serve as adjuncts, not primary therapy. Research consistently shows that delay in surgery for this population leads to worse long-term outcomes.
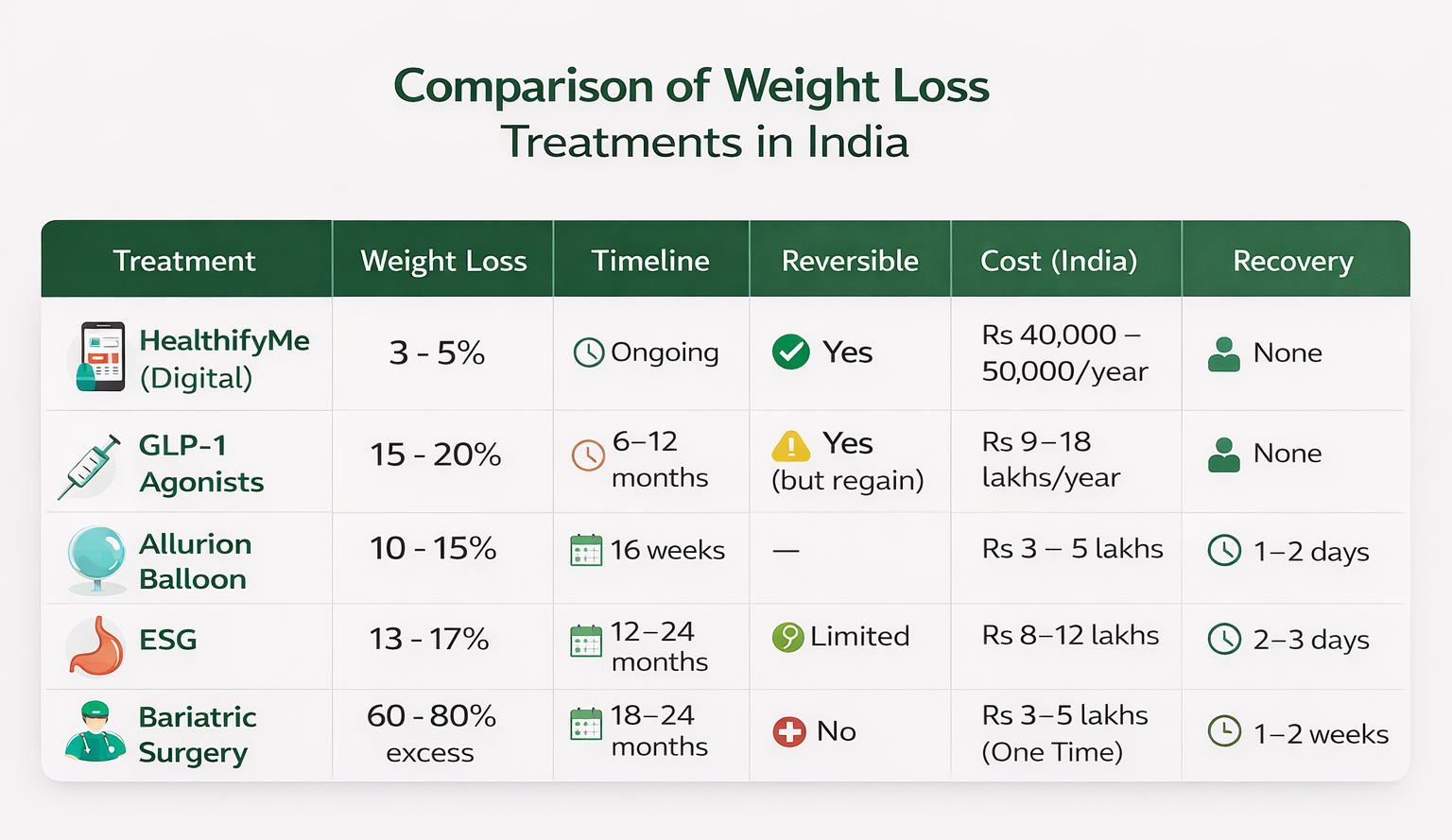
Comprehensive comparison table
Success requirements for any treatment
Regardless of which option you choose, certain fundamentals apply:
Nutritional foundations:
- Adequate protein intake (1.2-1.5g/kg body weight) to preserve muscle mass
- Resistance training alongside cardiovascular exercise
- Vitamin and mineral supplementation as indicated
Lifestyle factors:
- Sleep optimization targeting 7-8 hours nightly and addressing sleep apnea
- Stress management and mental health support
- Limiting alcohol consumption
Long-term commitment:
- Regular follow-up appointments (obesity management is not a "3-month project")
- Realistic expectations about plateaus, body composition changes, and the ongoing nature of maintenance
- Relapse prevention planning
- Support network engagement
Starting your obesity treatment journey with Fortis
The treatment ladder concept reflects a simple reality: obesity is a chronic disease requiring staged, personalized intervention. What works for one person may be inadequate for another. The key is matching treatment intensity to clinical need while building the habits that sustain results long-term.
For patients with severe obesity (BMI 35+), surgery remains the gold standard with proven outcomes that no other intervention matches. For those with milder obesity, medications and digital tools offer effective stepping stones. And for everyone, long-term follow-up determines whether initial weight loss becomes lasting transformation.
Fortis Healthcare offers a comprehensive approach to obesity treatment through its Metabolic & Bariatric Surgery program. The partnership with HealthifyMe at Fortis Hospital, Mohali bridges digital coaching with clinical care. Multidisciplinary teams including bariatric surgeons, endocrinologists, dietitians, and psychologists work together across accredited centers with documented clinical outcomes.
For more background on surgical approaches, the complete guide to obesity and bariatric surgery provides additional context for patients and families.
Ready to take the next step?
- Find a doctor specializing in obesity medicine or bariatric surgery
- Request a callback to schedule a consultation
- Explore health check packages for baseline metabolic assessment
Frequently asked questions about obesity control options
Q1: Which obesity control option is safest?
Safety depends on your individual health profile. Digital tools and lifestyle modification carry minimal physical risk but may be insufficient for severe obesity. GLP-1 medications (weight loss injections) are generally safe but contraindicated in patients with history of medullary thyroid cancer or MEN2. Bariatric surgery carries perioperative risk (mortality 0.03-0.2%), but for patients with BMI 35+ and comorbidities, the long-term health risks of untreated obesity typically exceed surgical risks. A thorough evaluation by your medical team determines which option balances safety and efficacy for your situation.
Q2: Will weight come back if I stop GLP-1 medications?
Clinical data shows 15-20% of weight lost returns upon discontinuation of GLP-1 agonists like semaglutide or tirzepatide. This reflects how these medications work: they regulate appetite through ongoing hormonal signaling. When the medication stops, appetite signals return to baseline. For this reason, many patients require lifelong therapy to maintain results, which has significant cost implications (Rs 75,000-1,50,000/month without insurance). Discuss with your physician whether GLP-1 therapy is intended as a temporary bridge or long-term maintenance.
Q3: Balloon vs ESG vs surgery: How do I choose among obesity control options?
The choice depends on your BMI, comorbidities, and readiness for permanent change. The Allurion Balloon (10-15% weight loss, 16 weeks, non-invasive) works best as a temporary jumpstart for BMI 27-35. ESG (13-17% weight loss, outpatient procedure) suits BMI 30-40 when you want procedural intervention without surgery. Bariatric surgery (60-80% excess weight loss, durable) is indicated for BMI 30+ with comorbidities or BMI 35+ regardless of comorbidities. Generally, higher BMI and more comorbidities point toward more intensive intervention.
Q4: What BMI or conditions usually trigger a bariatric surgery consult?
Standard guidelines recommend bariatric surgery consultation for BMI 35+ regardless of comorbidities, BMI 30-34.9 with serious obesity-related conditions (Type 2 diabetes, hypertension, sleep apnea, severe joint disease), and specifically for BMI 30-35 with uncontrolled Type 2 diabetes despite medical management. If you fall into any of these categories, a consultation with a bariatric surgery program helps clarify whether surgery is appropriate for your situation.
Q5: Can medications be used after bariatric surgery for weight regain?
Yes. GLP-1 agonists are increasingly used as adjunctive therapy for patients experiencing weight regain after bariatric surgery. Emerging evidence suggests synergistic effects between procedural and pharmacological approaches. This combination is typically considered when significant regain occurs despite dietary and exercise compliance. Your bariatric team can evaluate whether adding medication makes sense for your specific situation.
Q6: What does long-term follow-up look like after obesity treatment?
Long-term follow-up varies by treatment but is essential for all approaches. After bariatric surgery, expect visits several times yearly for the rest of your life, including nutritional assessment, lab work for micronutrient levels, weight monitoring, and adjustment of supplements. After ESG or balloon procedures, structured follow-up for at least 12-24 months ensures behavioral changes take hold. With GLP-1 medications, ongoing monitoring for side effects, efficacy, and metabolic parameters continues as long as therapy continues. For digital and lifestyle approaches, periodic check-ins help identify when escalation to more intensive treatment is needed. The common thread: obesity management is a long-term commitment, not a one-time fix.
Contact Us – Fortis Hospital Mohali
For appointments, consultations, and diagnostic services, please contact:
📞 72728 72728
Our care team will assist you with:
Doctor appointments
Diagnostic and screening services
Health check-ups
Call now to book your appointment at Fortis Hospital, Mohali.
Categories
Clear allMeet the doctor

- General Surgery | General Surgery | General and Minimal Access Surgery
-
 5 Years
5 Years
-
 1250
1250
Related Blogs
View all
Single Incision Laparoscopic Surgery (SILS) for Hernia Repair


Understanding Gallbladder Stones: Causes, Symptoms, and Treatment Options

Understanding Hernia - Causes, Symptoms, and Treatment Options

Gallstone Complications: When to Seek Medical Attention

Common Myths and Misconceptions About Bariatric Surgery

Understanding Appendicitis: Causes, Symptoms, Risk Factors & Treatment
Understanding Varicose Veins: Causes, Symptoms, Risk Factors & Treatment Options


FAQs

Keep track of your appointments, get updates & more!

