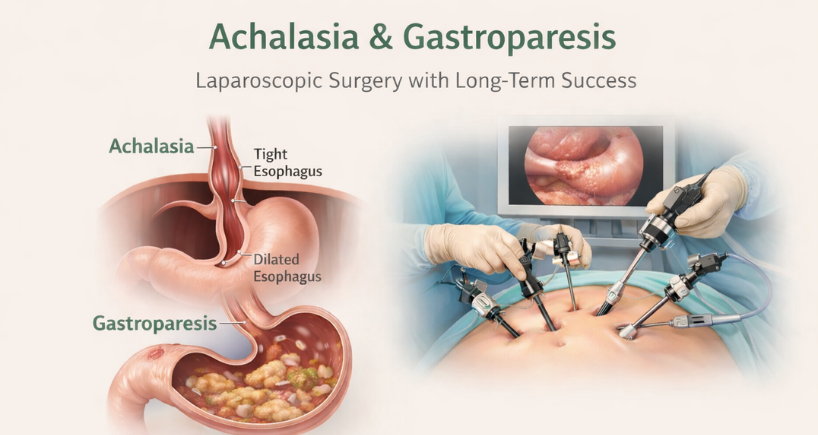






SURGICAL TREATMENT FOR ACHALASIA & GASTROPARESIS - The Gold Standard
Heller Myotomy with Anti-Reflux Protection | Pyloroplasty for Gastroparesis | Expert GI Surgeons Serving Tricity, Punjab & North India
Why Choose Surgery? The Definitive Treatment Approach
When you're diagnosed with achalasia (severe swallowing difficulty) or gastroparesis (slow stomach emptying), you'll hear about various treatment options — from medications and balloon dilation to newer endoscopic procedures like POEM. But there's one approach that has stood the test of time for over four decades: surgical treatment. At Fortis Hospital Mohali, our expert gastrointestinal surgeons specialize in laparoscopic surgical procedures that offer patients across Mohali, Chandigarh, Panchkula, Punjab, and North India the most comprehensive, durable solution with the lowest risk of long-term complications.
Surgery isn't just another option — for many patients, it's the gold standard that combines effectiveness, durability, and the crucial benefit of built-in reflux protection that endoscopic procedures cannot provide. Let me explain why surgical treatment may be the right choice for you.
Understanding Surgical Treatment: Two Proven Procedures
For Achalasia (Food Pipe Blockage): Laparoscopic Heller Myotomy with Fundoplication The laparoscopic Heller myotomy with fundoplication is considered the gold standard surgical treatment for achalasia worldwide. This procedure (often referred to by patients as food pipe surgery) has been refined over 40+ years and combines two critical components that work together to restore normal swallowing while preventing reflux.
What happens during the procedure:
- Minimally invasive approach — 4-5 small keyhole incisions (0.5-1 cm) in the abdomen, not large open cuts.
- Myotomy — the surgeon cuts the tight lower esophageal sphincter muscle (the valve at the bottom of the food pipe) under direct visualization, releasing the obstruction.
- Fundoplication — the upper part of the stomach is wrapped partially around the lower esophagus to create a new anti-reflux valve (to prevent severe heartburn and acid backup).
- Duration: 2-3 hours under general anesthesia.
The fundoplication component is what sets surgery apart from endoscopic POEM. While POEM simply cuts the muscle and leaves you vulnerable to reflux, surgical myotomy includes this protective wrap that prevents stomach acid from flowing back up — giving you the best of both worlds.
For Gastroparesis (Stomach Paralysis): Laparoscopic or Robotic Pyloroplasty For patients with gastroparesis (delayed stomach emptying) who haven't responded to medical management, pyloroplasty is a well-established surgical procedure that widens the pylorus (the valve between the stomach and small intestine) to improve gastric emptying (helping food leave the stomach faster).
Surgical approach:
- The pylorus is opened surgically and reconstructed to create a wider, more relaxed opening.
- Can be combined with gastric electrical stimulator implantation for severe cases.
- Direct visualization allows precise reconstruction for optimal long-term function.
Unlike G-POEM (the endoscopic alternative), surgical pyloroplasty allows complete reconstruction of the pyloric valve with suturing techniques that have been proven effective for decades.
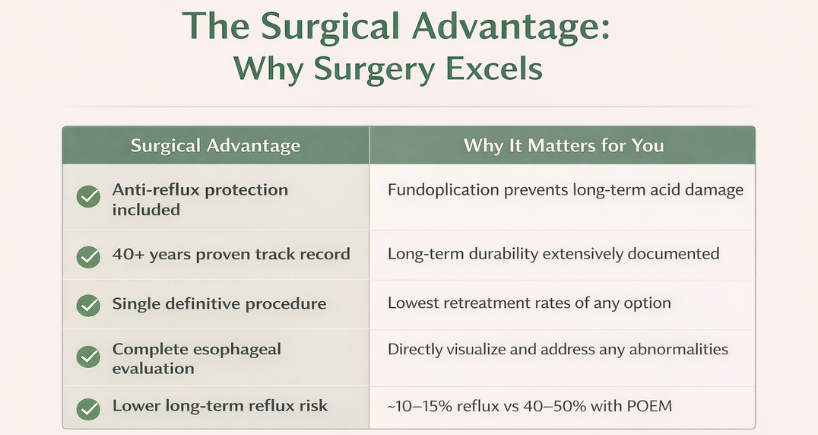
1. Built-In Reflux Protection: The Fundoplication Difference This is perhaps the most significant advantage. Achalasia patients who undergo Heller myotomy without fundoplication or choose POEM face a 40-50% risk of developing significant reflux. With surgical fundoplication, this risk drops to 10-15%.
Why this matters long-term:
- Chronic reflux isn't just uncomfortable — it causes esophagitis (inflammation), Barrett's esophagus (precancerous changes), and esophageal strictures.
- With surgery's built-in protection, you avoid decades of daily acid-suppressing medication.
- You eliminate the risk of long-term acid-related complications.
Think of it this way: POEM fixes your swallowing problem (food getting stuck in the chest) but creates a reflux problem. Surgery fixes your swallowing problem AND prevents reflux from becoming an issue. That's comprehensive care.
2. Four Decades of Proven Durability Laparoscopic Heller myotomy has been performed since the 1990s, and the open version dates back to the 1960s. We have extensive long-term data showing sustained effectiveness:
- 10-year success rates: 85-90% maintain excellent swallowing function.
- 15-year data: The majority of patients remain symptom-free without retreatment.
- Retreatment rates: Lowest among all achalasia treatments (5-10% over a lifetime).
While POEM is promising, we only have 10-15 years of data. Surgery has proven itself over multiple decades with millions of patients worldwide. That's the confidence of a truly established procedure.
3. Single Definitive Procedure with Lowest Retreatment Rates Pneumatic dilation requires repeat procedures every 1-3 years on average. Even POEM has 10-15% retreatment rates at 5 years. Surgical myotomy offers the highest likelihood of a single, definitive treatment that lasts a lifetime.
What this means practically:
- One recovery period instead of multiple procedures over the years.
- Lower lifetime healthcare costs despite higher initial investment.
- Peace of mind knowing you've addressed the problem comprehensively.
4. Direct Visualization and Comprehensive Evaluation During laparoscopic surgery, your surgeon directly visualizes the esophagus (food pipe), stomach, and surrounding structures. This allows:
- Detection and treatment of hiatal hernias (often coexisting with achalasia).
- Assessment of esophageal length and anatomy for optimal fundoplication type.
- Identification of any unexpected findings that might change management.
- Precise myotomy length tailored to your specific anatomy.
Endoscopic procedures work through a narrow tube and can't provide this comprehensive surgical evaluation.
5. Flexibility in Fundoplication Type: Personalized to You Not all anti-reflux wraps are the same. Experienced surgeons choose the fundoplication type based on your specific situation:
- Partial fundoplication (Dor or Toupet) — for most achalasia patients, maintains ability to burp and vomit.
- Complete (Nissen) fundoplication — rarely used in achalasia but available if needed for severe reflux risk.
- Tailored approach — your surgeon selects based on esophageal motility, anatomy, and reflux risk.
This customization ensures optimal outcomes for YOUR specific condition.
Laparoscopic Heller Myotomy: The Procedure Explained
Pre-Operative Preparation Before surgery at Fortis Mohali:
- Complete evaluation including manometry, endoscopy, and barium swallow.
- Pre-operative testing: blood work, chest X-ray, EKG.
- Liquid diet for 24-48 hours before surgery to empty the esophagus.
- NPO (nothing by mouth) after midnight before surgery.
- Bowel preparation may be recommended.
The Surgical Procedure Step-by-step surgical approach:
- General anesthesia — you're completely asleep and pain-free.
- Five small incisions (0.5-1 cm) in the upper abdomen.
- Laparoscope (camera) and specialized instruments inserted.
- Hiatal dissection — accessing the esophagus through the diaphragm.
- Myotomy — precisely cutting the esophageal and LES muscle for 6-8 cm, extending 2-3 cm onto the stomach.
- Fundoplication — wrapping the gastric fundus around the esophagus (Dor or Toupet technique).
- Hiatal hernia repair if present.
- Incisions closed with absorbable sutures.
Total surgical time: 2-3 hours. You'll spend 1-2 hours in recovery before being transferred to your hospital room.
What Makes Fortis Mohali's Surgical Program Exceptional
- High-volume center with experienced GI surgeons performing 50+ Heller myotomies annually.
- Advanced laparoscopic and robotic capabilities for optimal precision.
- Multidisciplinary team approach — surgeons, gastroenterologists, nutritionists working together.
- Comprehensive pre-operative evaluation ensuring appropriate patient selection.
- Standardized surgical protocols refined over hundreds of cases.
Recovery After Laparoscopic Heller Myotomy
Hospital Stay and Immediate Post-Op
- Hospital stay: 2-3 days typically.
- Pain management: Oral pain medication usually sufficient (laparoscopic approach causes less pain than open surgery).
- Early mobilization: Walk the same evening of surgery to prevent blood clots.
- Contrast swallow study on post-operative day 1-2 to confirm no leak.
- Clear liquid diet started after swallow study clears you.
Diet Progression After Surgery Structured advancement over 4-6 weeks:
- Week 1: Clear liquids (water, broth, clear juices).
- Week 2: Full liquids (smoothies, protein shakes, strained soups).
- Weeks 3-4: Soft foods (mashed potatoes, scrambled eggs, yogurt, tender fish).
- Weeks 4-6: Regular diet, introducing one new texture at a time.
By 6-8 weeks, most patients eat normally with no restrictions. Some surgeons recommend avoiding tough, dry meats and sticky rice initially, but most foods are well-tolerated.
Recovery Timeline What to expect:
- Week 1: Mild incisional pain, fatigue, some difficulty swallowing (temporary swelling).
- Week 2: Pain resolving, return to light activities, improved swallowing.
- Week 3-4: Return to desk work, most daily activities resumed.
- Week 6-8: Return to full activities including exercise and heavy lifting.
- 3 months: Full recovery, eating all foods comfortably.
Surgical Results: Long-Term Outcomes
Swallowing Improvement
- 85-90% of patients achieve excellent or good swallowing function.
- Eckardt symptom scores (validated questionnaire) improve by 75-85%.
- Weight gain and nutritional status improve significantly.
- Quality of life returns to near-normal for most patients.
Reflux Control The surgical advantage in numbers:
- Reflux symptoms: 10-15% with fundoplication vs 40-50% with POEM alone.
- Esophagitis on endoscopy: 5-10% vs 30-40% with POEM.
- Need for daily acid medication: <20% vs >60% with POEM.
This dramatic difference in reflux rates is why many surgeons still recommend surgery as first-line treatment, especially for younger patients who face decades of potential acid exposure.
Durability and Retreatment
- 10-year symptom control: 85-90% maintain relief.
- Lifetime retreatment rates: 5-10% require repeat intervention.
- When retreatment needed, options include pneumatic dilation or rarely repeat myotomy.
- Fundoplication remains intact long-term in >90% of patients.
Surgical Treatment for Gastroparesis: Pyloroplasty
When to Consider Surgery for Gastroparesis Unlike achalasia where surgery is first-line for many patients, gastroparesis surgery (treatment for food sitting in the stomach) is reserved for carefully selected cases:
- Refractory symptoms despite optimal medical management (diet, prokinetics, antiemetics).
- Objective evidence of delayed gastric emptying on scintigraphy.
- Evidence of pyloric dysfunction (high resistance on testing).
- No response to G-POEM or not a G-POEM candidate.
- Adequate gastric contractility (surgery doesn't help if the stomach is completely atonic).
Surgical Options Pyloroplasty techniques:
- Heineke-Mikulicz pyloroplasty — traditional, most common.
- Finney pyloroplasty — for more complex cases.
- Often combined with gastric electrical stimulator (GES) placement for refractory nausea/vomiting.
The procedure widens the pylorus surgically and reconstructs it with sutures to maintain the new wider configuration permanently.
Gastroparesis Surgery Outcomes Realistic expectations:
- 60-75% meaningful symptom improvement (similar to G-POEM but potentially more durable).
- Best results when combined with GES for nausea control.
- Long-term data more extensive than G-POEM.
- Allows for feeding jejunostomy tube placement if needed for nutritional support.
Surgery vs POEM: Making the Right Choice
Surgery May Be Your Best Option If:
- You're concerned about long-term reflux risk and want built-in protection.
- You prefer a single definitive procedure with the lowest retreatment rates.
- You value the 40+ years of proven long-term data.
- You have a hiatal hernia that needs repair (best done surgically).
- You're young and want to avoid decades of daily reflux medication.
- Your anatomy or prior surgeries make an endoscopic approach challenging.
Consider POEM Instead If:
- You want the fastest possible recovery (10-14 days vs 3-4 weeks).
- You're willing to manage reflux with long-term medication.
- You have Type III spastic achalasia (where POEM may offer advantages).
- You've had prior Heller myotomy and need retreatment.
- You prefer no visible scars (POEM is through the mouth).
The Honest Truth: Both Are Excellent At Fortis Mohali, we offer both surgical myotomy and POEM because both are excellent treatments with different trade-offs. The key is choosing the right one for YOUR priorities:
- Prioritize reflux prevention → Surgery
- Prioritize fastest recovery → POEM
- Prioritize long-term proven data → Surgery
- Prioritize no external scars → POEM
During your consultation, our multidisciplinary team (surgeons and gastroenterologists) will discuss both options honestly and help you make the choice that aligns with your values and circumstances.
Risks and Complications of Surgery
All procedures carry risks. Laparoscopic Heller myotomy is very safe in experienced hands, but you should know the potential complications:
Intraoperative Risks
- Esophageal or gastric perforation — rare (<1-2%), usually recognized and repaired immediately.
- Bleeding — rarely requires transfusion.
- Pneumothorax (air in chest cavity) — uncommon, usually resolves with observation.
Post-Operative Complications
- Difficulty swallowing (dysphagia or trouble passing food) in the first 1-2 weeks from swelling — expected and temporary.
- Incomplete myotomy requiring repeat procedure — 5-10%.
- Fundoplication too tight causing persistent dysphagia — 3-5%, may need revision.
- Reflux despite fundoplication — 10-15% develop some symptoms.
- Wound infection — very rare with the laparoscopic approach.
Long-Term Issues
- Fundoplication breakdown over time — uncommon but possible, reflux may recur.
- Gas-bloat syndrome — difficulty burping or vomiting (5-10% with complete wrap, less with partial).
- Recurrent symptoms requiring retreatment — 5-10% over a lifetime.
Overall complication rates at high-volume centers like Fortis Mohali are <5% for major complications, making this a very safe procedure.
Frequently Asked Questions About Surgery
Is laparoscopic surgery really minimally invasive? Yes. While it requires general anesthesia and abdominal incisions, the incisions are only 0.5-1 cm. This results in significantly less pain, faster recovery, and better cosmetic results than open surgery. Most patients are surprised at how manageable post-operative pain is.
Will I have visible scars? You'll have 4-5 small scars in the upper abdomen, typically 0.5-1 cm each. They fade significantly over time and are barely noticeable for most patients. If scarring is a major concern, POEM leaves no external scars.
How long until I can eat normally? Most patients eat a regular diet by 6-8 weeks. Some foods (tough meats, sticky rice) may be challenging initially, but tolerance improves over time. By 3 months, nearly all patients eat everything without restrictions.
What if the surgery doesn't work? If symptoms persist or recur, options include: pneumatic dilation (effective in many post-surgical recurrences), POEM (can be done after Heller myotomy), or rarely repeat surgical myotomy. The vast majority of patients achieve lasting relief.
Can I have surgery if I had POEM before? Yes. If POEM didn't provide adequate relief or symptoms recurred, laparoscopic Heller myotomy with fundoplication can still be performed. Your surgeon will assess whether the prior POEM affects the surgical approach.
Does insurance cover surgical treatment? Yes. Laparoscopic Heller myotomy is a well-established, proven procedure covered by most insurance plans in India. Our team at Fortis Mohali helps navigate insurance approval.
Why Choose Fortis Mohali for Surgical Treatment?
Our surgical expertise includes:
- High-volume GI surgery program with dedicated esophageal surgeons.
- Advanced laparoscopic and robotic surgical platforms.
- Multidisciplinary approach — surgeons work closely with gastroenterologists.
- Comprehensive pre-operative evaluation and patient selection.
- Standardized surgical protocols proven over hundreds of cases.
- Complete spectrum of care: medical management, POEM, and surgery under one roof.
At Fortis Mohali, you're not pushed toward one treatment or another. We honestly discuss all options — medical management, pneumatic dilation, POEM, and surgery — and help you choose what's right for YOUR situation. Our goal is your best long-term outcome, not promoting any particular procedure.
Proven. Durable. Comprehensive. Surgical treatment offers the gold standard for achalasia and gastroparesis with built-in reflux protection.
Schedule Your Surgical Consultation
If you're considering surgical treatment for achalasia or gastroparesis, schedule a consultation with our GI surgery team at Fortis Mohali. We'll conduct a thorough evaluation, discuss all treatment options, and develop a personalized plan that aligns with your goals and priorities.
Surgery has helped millions of patients worldwide achieve lasting relief with comprehensive anti-reflux protection. Let our experienced team determine if it's the right choice for you.
Contact Us – Fortis Hospital Mohali
For appointments, consultations, and diagnostic services, please contact:
📞 72728 72728
Our care team will assist you with:
Doctor appointments
Diagnostic and screening services
Health check-ups
Call now to book your appointment at Fortis Hospital, Mohali.
Categories
Clear allMeet the doctor

- General Surgery | General Surgery | General and Minimal Access Surgery
-
 5 Years
5 Years
-
 1250
1250
Related Blogs
View all
Single Incision Laparoscopic Surgery (SILS) for Hernia Repair


Understanding Gallbladder Stones: Causes, Symptoms, and Treatment Options

Understanding Hernia - Causes, Symptoms, and Treatment Options

Gallstone Complications: When to Seek Medical Attention

Common Myths and Misconceptions About Bariatric Surgery

Understanding Appendicitis: Causes, Symptoms, Risk Factors & Treatment
Understanding Varicose Veins: Causes, Symptoms, Risk Factors & Treatment Options


FAQs

Keep track of your appointments, get updates & more!

