






Targeted Therapy: Attacking Cancer’s Molecular Weak Spots
By Dr Rajeev Bedi | Director, Medical Oncology | Fortis Cancer Institute, Mohali
Precision oncology has revolutionized how we treat cancer, moving away from treating a tumor based on its location in the body to targeting its specific molecular drivers. The most transformative result of this principle is targeted therapy—drugs that "think before they act.
"These are drugs that do not carpet-bomb the body the way traditional chemotherapy does. They identify the specific molecular abnormality fuelling the cancer and shut it down — precisely, selectively, and often with dramatically fewer side effects."
If your oncologist mentions terms like genomic testing, molecular profiling, or “actionable mutations,” they are looking to see if targeted therapy is right for you.
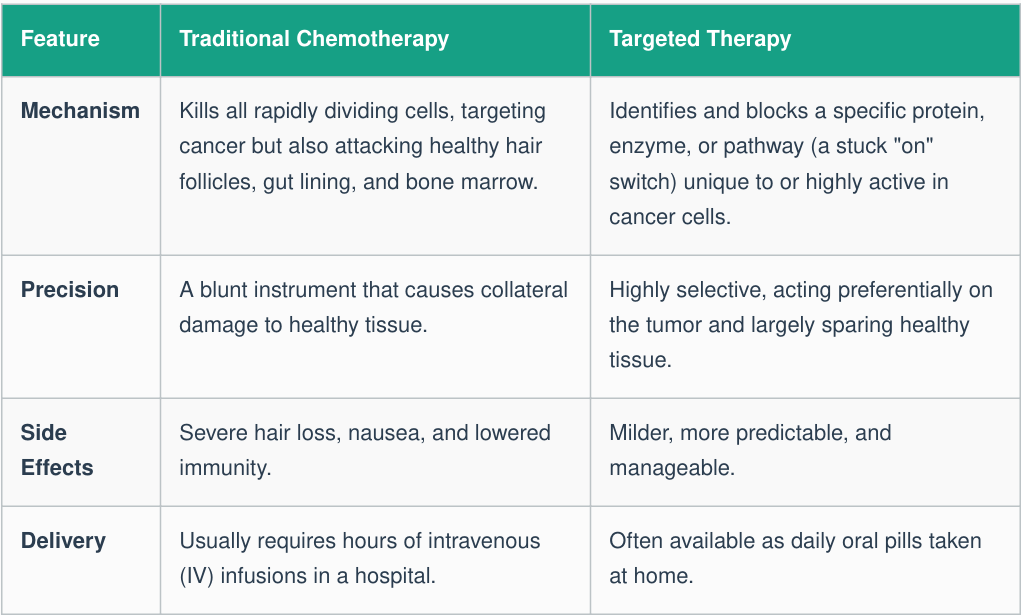
Chemotherapy vs. Targeted Therapy: A Fundamental Difference
The difference between these two treatments is in their very nature, not just their degree of effectiveness.
How It Works: The Lock-and-Key Principle
Cancer cells survive due to abnormal molecular signals, such as mutated genes creating permanently activated proteins or overexpressed receptors capturing too many growth signals. Sometimes, fusion genes create entirely new proteins that drive uncontrolled growth. Each of these vulnerabilities acts as a molecular "lock". Molecular profiling is the process of finding that lock, and targeted therapy provides the exact "key" to switch it off.
The Four Major Classes of Targeted Therapy
1. Tyrosine Kinase Inhibitors (TKIs)
TKIs are small-molecule oral medications that can be taken at home. They work by blocking tyrosine kinases—enzymes that function as continuously activated molecular switches inside cancer cells, driving uncontrolled growth.
Key Points:
- Taken orally (pill form)
- Highly specific to certain genetic mutations
- Require molecular testing before treatment
Examples:
- Osimertinib – EGFR-mutant lung cancer
- Alectinib – ALK-rearranged lung cancer
- Imatinib – BCR-ABL-positive Chronic Myeloid Leukemia (CML)
Important: These therapies only work when the targeted molecular abnormality is present, making biomarker testing essential before treatment.
2. Monoclonal Antibodies
Monoclonal antibodies are laboratory-engineered proteins administered through intravenous (IV) infusion, typically every 2–4 weeks. They target specific proteins on the surface of cancer cells.
How They Work:
- Block growth-promoting receptors
- Mark cancer cells for destruction by the immune system
- Interfere with tumor blood supply
- Deliver therapeutic agents to cancer cells
Examples:
- Trastuzumab – Targets HER2-positive breast cancer
- Bevacizumab – Inhibits blood vessel formation that tumors need to grow
3. Antibody-Drug Conjugates (ADCs)
ADCs are often described as "guided missiles" in cancer therapy. They combine the precision targeting of monoclonal antibodies with the cell-killing power of chemotherapy.
How They Work:
- The antibody identifies and binds to a specific cancer cell.
- The complex is absorbed into the cell.
- A potent cytotoxic drug ("warhead") is released directly inside the cancer cell.
- Cancer cells are destroyed while minimizing damage to healthy tissues.
Example:
- Trastuzumab Deruxtecan (T-DXd) – A breakthrough therapy for:
- HER2-positive breast cancer
- HER2-low breast cancer
- HER2-mutant lung cancer
4. Signal Pathway Inhibitors
These therapies target critical intracellular signaling pathways that cancer cells rely on for growth, survival, and division.
How They Work:
- Interrupt downstream molecular signaling networks
- Prevent cancer cell proliferation
- Exploit specific weaknesses in tumor biology
Examples:
- CDK4/6 Inhibitors – Used in hormone receptor-positive breast cancer
- PARP Inhibitors – Effective in BRCA-mutated cancers by targeting defects in DNA repair mechanisms
Clinical Benefit: These therapies can significantly improve disease control while often causing fewer side effects than traditional chemotherapy.
Expanding the Target List
Not all cancers have actionable targets, but the list expands yearly. Lung cancer leads the field, with 60–70% of patients having a targetable mutation. Targets once thought "undruggable," like KRAS mutations, are now treatable with drugs like sotorasib. Furthermore, precision oncology is increasingly "tumour-agnostic," meaning drugs like larotrectinib can treat NTRK fusions across lung, thyroid, or colon cancers equally—treating the mutation, not the organ.
The Treatment Experience and Side Effects
What Patients Can Expect During Treatment
Starting an oral targeted therapy is very different from traditional cancer treatment. Unlike conventional chemotherapy, there is usually no need for a chemotherapy port, prolonged hospital visits, or extended infusion sessions. Patients simply take their prescribed medication at home and visit their oncologist periodically for monitoring, blood tests, and treatment assessment.
While targeted therapies are generally better tolerated than conventional chemotherapy, they are not completely free of side effects. Importantly, these side effects are often predictable and directly related to the biological pathway being targeted.
Common Side Effects by Therapy Type
EGFR Inhibitors
- Acne-like skin rash
- Diarrhea
- Usually manageable with supportive medications and dose adjustments
ALK Inhibitors
- Visual disturbances
- Elevated liver enzymes
- Require regular liver function monitoring
HER2-Targeted Antibodies
- Potential effects on heart function
- Require routine cardiac monitoring with echocardiography every 3 months
CDK4/6 Inhibitors and PARP Inhibitors
- Low blood cell counts
- Fatigue
- Regular blood tests help detect and manage these effects early
TKIs for Chronic Myeloid Leukemia (CML)
- Fluid retention
- Muscle cramps
- Usually manageable with supportive care and treatment modifications when necessary
Quality of Life During Treatment
One of the greatest advantages of targeted therapy is its ability to control cancer while allowing many patients to maintain a normal lifestyle. Most individuals can continue working, exercising, traveling, and participating in daily activities throughout treatment. With regular monitoring and proactive management of side effects, targeted therapies often provide an effective balance between cancer control and quality of life.
Key Message: Targeted therapy is not simply a treatment—it is a long-term, personalized approach to cancer care that aims to maximize effectiveness while minimizing disruption to everyday life.
The Challenge of Resistance
Eventually, biology takes over: cancer cells can evolve under pressure and develop secondary mutations or bypass pathways, causing the drug to stop working. However, this is not a failure. Oncologists perform new molecular profiling, often through a simple "liquid biopsy" blood test, to find the resistance mechanism. We can then switch the patient to a next-generation drug designed to overcome that specific mutation (e.g., using osimertinib for T790M resistance).
"Resistance is not the end of precision oncology. It is precision oncology working in real time — adapting the treatment to the tumour’s evolution..."
A Real-Life Example
A 52-year-old non-smoking woman from Amritsar with advanced lung adenocarcinoma avoided harsh chemotherapy when genomic testing revealed an ALK rearrangement (found in ~5% of such cancers). Treated with a daily ALK inhibitor pill, her tumor shrank by 60% in two months. Fourteen months later, she is living normally, cooking, and attending school events—all without a single dose of chemotherapy.
5 Questions to Ask Your Oncologist
- Has molecular profiling been done on my tumor, and if not, should it be?
- Does my cancer have an actionable mutation that can be treated with a targeted therapy?
- Is targeted therapy an option instead of, or alongside, chemotherapy?
- What are the specific side effects of the recommended targeted therapy, and how are they managed?
- If the targeted therapy stops working, will repeat molecular testing help guide the next treatment approach?
Categories
Clear allMeet the doctor

- Oncology | Medical Oncology
-
 27 Years
27 Years
-
 2550
2550
Related Blogs
View all









FAQs
Does every patient need it?
No. It only works if a specific molecular target is found;
otherwise, chemotherapy or immunotherapy may be more appropriate.Can it cure cancer?
It can produce cure-like remissions in some cancers (like CML), but in advanced solid tumors, it typically controls the disease for months or years, significantly extending survival

Keep track of your appointments, get updates & more!

