






TAVR for Bicuspid Aortic Valve Disease New Evidence and Outcomes
Bicuspid Aortic Valve disease has always been a bit of an outlier. The valve forms with two leaflets instead of three, and that simple anatomic difference leads to asymmetric calcification, unusual annular shapes, and sometimes dilation of the aortic root. For a long time, that made percutaneous valve replacement technically tricky; surgeons preferred open replacement for predictable results. Over the last few years, though, device design and imaging have improved enough that the TAVR procedure is a realistic option for an increasing number of patients with bicuspid anatomy. The change is careful, not sudden, and patient selection remains the central question.
Most teams treat bicuspid cases with extra caution. Outcomes have improved in experienced centres, but some risks remain higher than for tricuspid valves. The practical task for clinicians and patients is to weigh those trade-offs in light of age, comorbidity, anatomic detail and personal priorities. When chosen thoughtfully, TAVR can shorten recovery time and reduce immediate procedural stress compared with classical surgical routes.
Why Bicuspid Anatomy Presents Unique Challenges
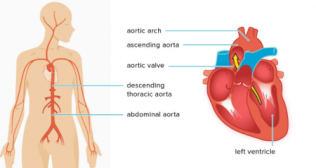
A bicuspid valve typically shows more eccentric calcium deposits and a non circular annulus. That matters because a transcatheter valve depends on predictable radial expansion and a reliable seal. When calcium sits unevenly, the valve frame may not expand symmetrically and small gaps can permit paravalvular leak. The ascending aorta around the valve is also sometimes aneurysmal or less compliant, adding another layer of complexity.
Another practical issue is that imaging measurements must be precise. CT planning is not optional. Teams spend more time mapping annular dimensions and calcium distribution than they would for a tricuspid valve. That careful planning often pays off in better procedural control.
What Recent Studies Are Showing
Registry data and newer cohort studies now report better technical success than earlier series. In experienced hands, procedural success rates are approaching those seen in tricuspid valves for selected patients. Rates of moderate to severe paravalvular leak have fallen with improved sizing, valve choice and post dilation techniques. Early mortality and stroke rates are generally comparable in recent reports, though longer term durability data for bicuspid patients remains more limited.
A few consistent trends emerge from the evidence:
- Device iteration and operator experience matter greatly.
- Paravalvular leak is less common than it used to be, but still slightly more likely than with tricuspid valves.
- Pacemaker rates vary by device and implantation depth, and are an important talking point with patients.
None of these findings imply that TAVR is always better. They simply show the balance is shifting for certain subsets of patients.
Who Makes a Good Candidate
Not every bicuspid valve is suitable for TAVR. Good candidates tend to have:
- Age or comorbidity that increases surgical risk
- Annular geometry that allows predictable valve expansion on CT
- No severe aortopathy that would need surgical root or ascending aorta repair
- Calcium distribution that does not predict malapposition or leaflet rupture
Patients who are younger, fit and have associated aortic root disease still usually do better with surgical aortic valve replacement. The decision is a multidisciplinary one. Cardiac surgeons, interventional cardiologists and imaging specialists together evaluate the imaging and the clinical context, then advise what is safest and most durable for the individual.
Procedural Considerations That Affect Outcomes
Several technical steps reduce the chance of complications.
- High resolution CT planning guides valve sizing and orientation.
- Pre-dilation with a balloon can test annular compliance before final valve deployment.
- Precise implantation depth minimizes conduction system injury and reduces pacemaker necessity.
- Post dilation helps improve valve expansion and reduce paravalvular leak when safe to perform.
Operators also choose valve type based on the anatomy. Some valve platforms conform better to eccentric calcification. Others provide easier recapture or repositioning. Experience with specific devices in bicuspid anatomy tends to shorten the learning curve and improve consistency.
What TAVR Procedure Recovery Looks Like in Bicuspid Cases
Recovery after TAVR tends to be faster than after open surgery for most patients. Mobility often resumes within 24 to 48 hours. Hospital stays are frequently shorter, and pain is usually less intense because there is no sternotomy. That said, bicuspid cases may require slightly closer early monitoring for conduction disturbances and valve performance.
Typical recovery milestones are:
- Early mobilisation within the first day when uncomplicated.
- Echocardiography before discharge to assess valve function and detect leak.
- Rhythm monitoring for several days; pacemaker implantation is uncommon but not rare.
- Gradual increase in activity over weeks with cardiology follow up.
The recovery pathway is familiar to most cardiology teams, but it is tailored to the individual’s pre procedure fitness and intra procedural course.
Risks to Discuss Honestly
Some risks are shared with tricuspid TAVR; others are relatively increased in bicuspid settings.
Key risks include:
- Paravalvular Regurgitation, which can be mild to moderate and sometimes requires reintervention.
- Need for Permanent Pacemaker due to conduction block.
- Vascular complications at the access site when transfemoral approach is used.
- Rare annular or aortic injury if calcification is extreme.
Durability remains the open question. Long term valve function in bicuspid anatomy is under active study. The available data suggests reasonable short to mid term performance, but younger patients may still favour surgery because the evidence for long term durability of surgical valves is more mature.
Comparing TAVR and TAVR Surgery Alternatives
Consideration
TAVR
Surgical Aortic Valve Replacement
Invasiveness
Less invasive, shorter initial recovery
More invasive, longer recovery but established durability
Suitability in bicuspid
Increasingly feasible in selected patients
Preferred for complex anatomy or younger patients
Reintervention risk
Slightly higher if leak or malposition occurs
Lower when valve and root reconstruction are needed
Hospital stay
Often 1 to 3 days
Typically longer, variable by centre
This summary helps frame choices but each case needs bespoke discussion.
How Decisions Are Made Practically
Multidisciplinary heart team meetings are the right setting. They combine CT imaging, surgical assessment and patient preferences. Topics that move the decision one way or another include patient age, life expectancy, coexisting aortic disease and patient tolerance for potential reintervention. Shared decision making helps patients understand trade offs rather than choosing on a single metric.
Final Closing Summary
TAVR for bicuspid aortic valve disease is no longer an experiment for every case. It is a carefully considered option for selected patients, especially older individuals or those at elevated surgical risk whose anatomy looks favourable on detailed CT planning.
Outcomes have improved with better devices and more experienced operators, but the approach is not without additional considerations compared with tricuspid valves. Honest discussion about paravalvular leak, pacemaker risk and long term durability is essential. For anyone facing this choice, seek a multidisciplinary evaluation that explains how anatomy, life expectancy and personal goals shape the best path forward.
Categories
Clear allRelated Blogs
View all







FAQs

Keep track of your appointments, get updates & more!

