





Understanding Extrahepatic Biliary Atresia in Newborns - A Guide for Parents and Key Insights for Paediatricians
A Guide for Parents and Key Insights for Paediatricians
By Dr Sandeep Jaglan | Consultant, Pediatric Surgery | Fortis Hospital, Mohali
When Jaundice Does Not Go Away: A Parent’s Alarm Bell
Newborn jaundice (yellowing of the skin and eyes) is extremely common and usually harmless—most babies recover within the first week or two with simple measures like sunlight or phototherapy (a special blue-light treatment). But what if the yellow tint in your baby’s skin and eyes does not fade after two weeks? What if the stools turn pale, almost chalk-white, and the urine looks unusually dark?
These subtle but critical signs could point to extrahepatic biliary atresia (EHBA) — a rare yet serious liver condition where the bile ducts (tiny tubes that drain bile from the liver) outside the liver are blocked or absent. EHBA affects roughly 1 in 10,000 to 20,000 newborns globally, with a higher incidence reported across parts of Asia, including India. It is the leading cause of liver-related death in children and remains the most common reason for paediatric liver transplantation worldwide.
Recently, our paediatric surgical team at Fortis Hospital Mohali successfully operated on a 40-day-old baby diagnosed with extrahepatic biliary atresia. This case reinforced a truth we see time and again: early detection saves livers and lives. Through this article, I want to help parents across Chandigarh, Punjab, and North India recognise the warning signs early and give paediatricians a concise clinical reference for timely referral.
What Exactly Is Extrahepatic Biliary Atresia?
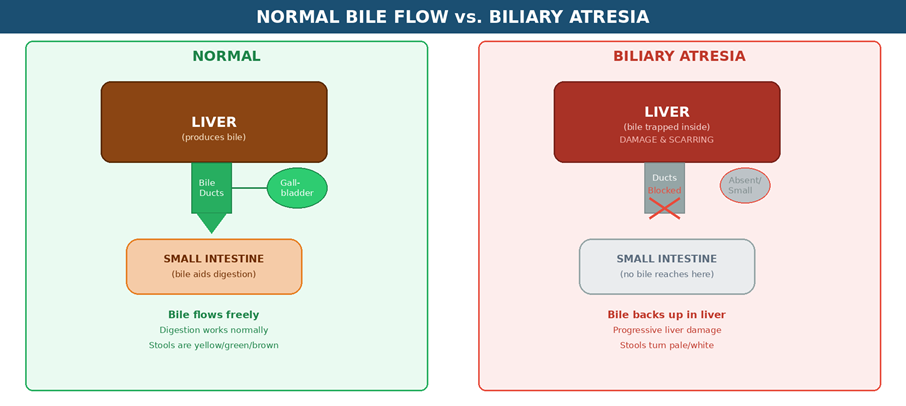
Think of bile ducts as tiny pipes that carry bile — a digestive fluid produced by the liver — down to the small intestine. Bile helps your baby digest fats and absorb essential fat-soluble vitamins (A, D, E, and K). It also carries waste products out of the liver.
In EHBA, the bile ducts outside the liver become scarred, blocked, or are entirely absent. With nowhere to go, bile backs up inside the liver, triggering inflammation and progressive scarring (a condition called cirrhosis — permanent liver damage from repeated scarring). If left untreated, this damage can lead to complete liver failure within the first few years of life.
The condition typically becomes apparent within the first two to eight weeks after birth. About 80 to 90 percent of cases are the perinatal type, developing after birth, while a smaller proportion are embryonic in origin and may occur alongside other birth defects involving the heart or spleen.
Important: The exact cause of EHBA remains unknown. Researchers believe it may involve a combination of genetic predisposition, immune system abnormalities, viral triggers, or environmental factors. No parent is at fault for this condition.
Red Flags Every Parent Should Know
This is perhaps the most important section of this article. Recognising these early warning signs can make the difference between saving your baby’s native liver and needing a transplant.
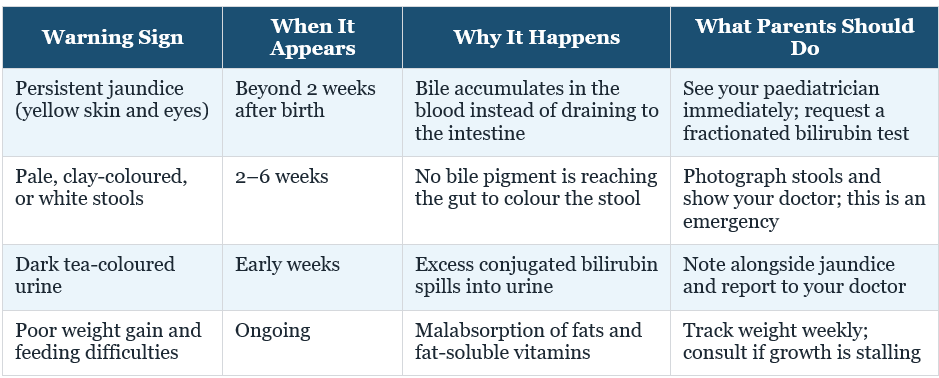
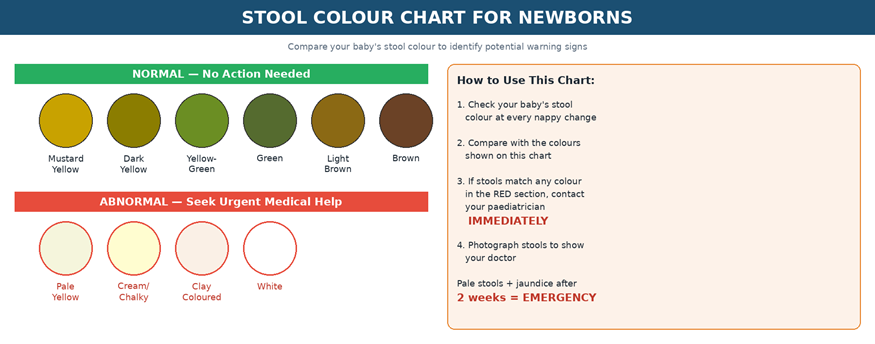
The stool colour rule is your single most powerful screening tool at home. Healthy baby stools are mustard yellow, green, or brown. Chalky white, pale yellow, or clay-coloured stools in a jaundiced newborn are a medical emergency. Parents across the Tricity region and Punjab should not adopt a wait-and-watch approach.
The 60-Day Golden Window: Why Every Day Counts
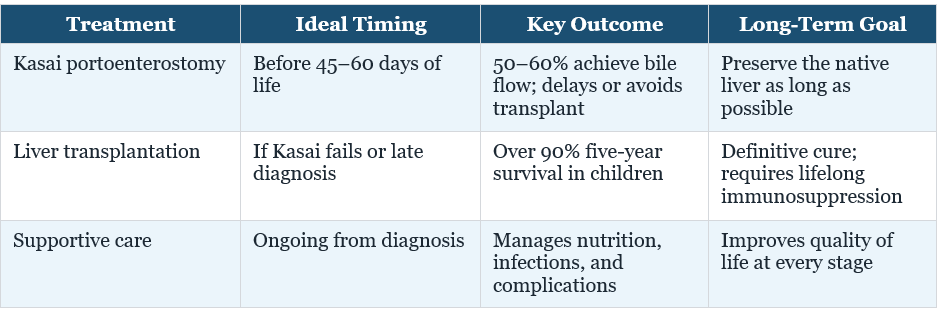
The primary surgical treatment for EHBA — the Kasai portoenterostomy (a surgery that creates a new pathway for bile to drain from the liver into the intestine) — works best when performed within the first 45 to 60 days of life. Research consistently shows that bile flow is successfully restored in approximately 50 to 60 percent of infants operated on within this window. Beyond 90 days, the success rate drops dramatically, and irreversible biliary cirrhosis (permanent liver scarring from bile blockage) often sets in.
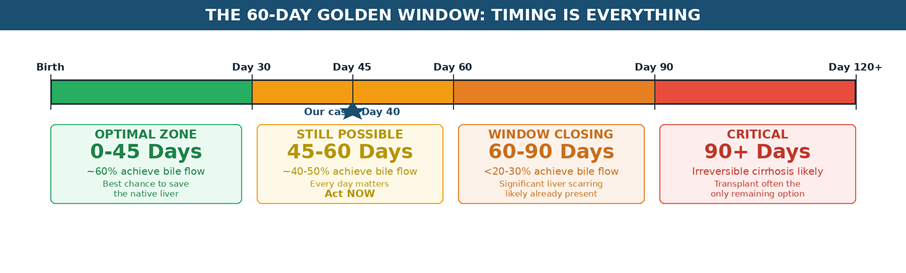
In our recent case at Fortis Mohali, we were able to perform the Kasai procedure on a 40-day-old infant—well within the golden window—because the parents acted quickly on the early signs and the referring paediatrician made a prompt referral. That kind of awareness and teamwork is exactly what saves native livers.
How Is EHBA Diagnosed?
Diagnosing biliary atresia requires a structured, step-by-step evaluation. Here is what the typical diagnostic pathway looks like:
Blood tests: Elevated direct (conjugated) bilirubin — a specific form of the yellow waste pigment that indicates bile is not draining properly — is the first biochemical clue. If the direct bilirubin exceeds 1 to 2 mg/dL in a jaundiced infant, further evaluation is mandatory.
Abdominal ultrasound: Looks for a small or absent gallbladder, the triangular cord sign (a specific ultrasound finding near the liver) at the liver hilum (the area where blood vessels and ducts enter the liver), and helps rule out other causes like a choledochal cyst (a different type of bile duct swelling that is treatable).
Hepatobiliary scintigraphy (HIDA scan): A nuclear imaging study (a special scan using a small, safe amount of radioactive tracer) where a tracer is injected. In EHBA, the liver takes up the tracer normally but fails to excrete it into the intestine.
Liver biopsy: A tiny sample of liver tissue is taken with a needle and examined under a microscope. It reveals characteristic bile duct proliferation (abnormal growth of tiny bile ducts) and portal fibrosis (scarring around the bile duct areas).
Intraoperative cholangiogram: The definitive gold standard. During surgery, contrast dye (a special dye visible on X-ray) is injected into the bile duct remnant to confirm whether bile reaches the intestine.
Diagnosis often requires evaluation at a specialised paediatric hepatology or surgical centre. For families in Mohali, Chandigarh, Panchkula, and the wider Punjab region, early referral to such a centre can save precious days.
Treatment: The Kasai Procedure and Beyond
The Kasai Portoenterostomy

Named after the Japanese surgeon who pioneered it, the Kasai procedure involves removing the damaged, scarred bile ducts and directly connecting a loop of the small intestine to the liver surface (the porta hepatis — the “doorway” of the liver where ducts and blood vessels enter). This creates a new pathway for bile to drain from the liver into the gut.
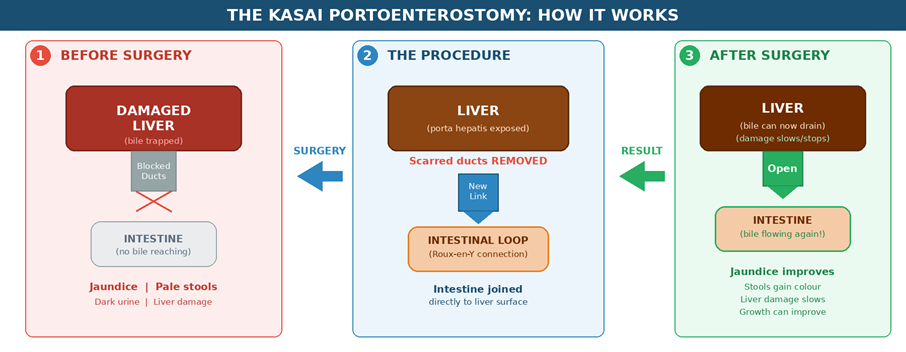
This is a highly delicate and technically demanding surgery, particularly in tiny newborns. Post-operative care includes antibiotics to prevent cholangitis (infection of the bile drainage system — a common complication after the Kasai procedure), ursodeoxycholic acid (a medication that supports bile flow), and supplementation with fat-soluble vitamins A, D, E, and K along with nutritional support.
When a Liver Transplant Becomes Necessary
Despite a successful Kasai procedure, a significant proportion of children—estimates suggest 70 to 80 percent—will eventually require a liver transplant, often by the age of one to two years if the initial surgery does not achieve adequate bile drainage. Some children with a good Kasai outcome can preserve their native liver for years or even decades, but long-term follow-up remains essential.
The reassuring news is that paediatric liver transplantation today has excellent outcomes, with over 90 percent five-year survival rates. In India, living-donor transplants (where a parent or close relative donates a portion of their liver) are common and highly successful. At Fortis Mohali, families have access to the full continuum of care—from the initial Kasai procedure through to complex liver transplantation—so you never have to change hospitals as your child’s needs evolve.
Life After Treatment: What to Expect
Children treated for biliary atresia need regular, lifelong follow-up. This includes periodic blood tests to monitor liver function, ultrasound imaging, nutritional assessments, and vigilance for complications like cholangitis (bile duct infection) or portal hypertension (high blood pressure in the veins carrying blood from the intestines to the liver, which can cause internal bleeding).
With proper medical care, many children with EHBA grow, attend school, play, and lead active, fulfilling lives. Nutritional support—including high-calorie formulas and vitamin supplementation—plays a crucial role in ensuring healthy growth. Advances in both surgical techniques and transplant medicine mean that outcomes for children with biliary atresia are better today than at any point in history.
Clinical Note for Paediatricians
This section offers quick-reference guidance for primary care providers and referring paediatricians.
- Screen every infant with jaundice persisting beyond 14 days using fractionated (direct and indirect) bilirubin—not just total bilirubin.
- A direct bilirubin level exceeding 1 to 2 mg/dL (or more than 20 percent of total bilirubin) warrants immediate referral to a paediatric hepatologist or surgeon.
- Stool colour monitoring in the first month is a simple, cost-effective screening tool. Consider providing parents with a stool colour card at the time of discharge.
- Do not delay diagnostic workup. Time sensitivity cannot be overstated: Kasai outcomes decline steeply after 60 days, and by 90 days, native liver salvage becomes unlikely.
- Post-Kasai patients need close surveillance with serial liver function tests, abdominal ultrasound, and prompt management of cholangitis episodes.
- A multidisciplinary team—paediatric surgeon, hepatologist, gastroenterologist, nutritionist, and transplant specialists—delivers the best outcomes. Early referral to a tertiary centre is the single most impactful step a primary care physician can take.
A Word to Parents: You Are Not Alone
Receiving a diagnosis of biliary atresia for your newborn can feel overwhelming and frightening. It is natural to feel anxious, guilty, or uncertain. Please remember that this condition is not caused by anything you did or did not do during pregnancy. The most important thing you can do is act quickly on the warning signs and trust your medical team.

Support groups, genetic counselling, and mental health resources can be invaluable as you navigate your child’s treatment journey. Many families who have walked this path will tell you that with the right medical care, children with biliary atresia go on to thrive.
Act Early, Act Now
For parents: If your newborn’s jaundice has not resolved by two weeks, or if you notice pale stools and dark urine, do not wait. Seek medical evaluation immediately. Time is liver tissue.
For paediatricians: Early referral is the single most important determinant of native liver survival. Partner with specialised centres for rapid evaluation. Every day of delay narrows the golden window.
At Fortis Hospital Mohali, our paediatric surgical team is committed to providing advanced, compassionate care for the smallest and most complex patients. If you suspect biliary atresia, reach out to our Paediatric Surgery or Paediatric Gastroenterology department for an urgent consultation.
Disclaimer: This article is for educational and awareness purposes only and is not a substitute for professional medical advice. Always consult a qualified healthcare provider for diagnosis and treatment.
About the Author
Dr Sandeep Jaglan is a Consultant in Pediatric Surgery at Fortis Hospital, Mohali. He specialises in advanced neonatal and paediatric surgical care, including the management of complex hepatobiliary conditions in newborns and children.
Contact Us – Fortis Hospital Mohali
For appointments, consultations, and diagnostic services, please contact:
📞 72728 72728
Our care team will assist you with:
Doctor appointments
Diagnostic and screening services
Health check-ups
Call now to book your appointment at Fortis Hospital, Mohali.
Categories
Clear allMeet the doctor

- Paediatrics | Paediatric Surgery
-
 7 Years
7 Years
-
 1250
1250
Related Blogs
View all






FAQs
Is biliary atresia caused by something I did during pregnancy?
Absolutely not. Biliary atresia is not caused by anything a mother did or did not do during pregnancy. It is not inherited, not contagious, and not preventable. The exact cause remains unknown, though researchers believe a combination of immune, viral, and possibly genetic factors may be involved. No parent should feel guilt about this diagnosis.
What is the survival rate for babies with biliary atresia?
With timely Kasai surgery (ideally before 60 days), approximately 50–60% of infants achieve bile flow and can delay or avoid a liver transplant for years or even decades. When a liver transplant is eventually needed, paediatric transplant outcomes are excellent—over 90% five-year survival. The key factor is how early the condition is detected and treated.
How can I tell the difference between normal newborn jaundice and biliary atresia?
Normal newborn jaundice (also called physiological jaundice) appears in the first few days of life and resolves within 1–2 weeks. In biliary atresia, jaundice persists or deepens beyond 2 weeks. The most important clue is stool colour: normal baby stools are yellow, green, or brown. Pale, clay-coloured, or white stools alongside persistent jaundice and dark urine are red flags requiring immediate medical evaluation.
What is the Kasai procedure? Is it safe for such a tiny baby?
The Kasai portoenterostomy is a well-established, life-saving surgery where the blocked bile ducts are removed and a loop of the baby’s own intestine is connected directly to the liver, creating a new drainage pathway for bile. Yes, it is performed on very young, very small newborns—and that is precisely why it should be done at a specialised centre with experienced paediatric surgeons. The younger the baby at the time of surgery (ideally under 60 days), the better the outcome.
Will my child need a liver transplant even after the Kasai procedure?
Possibly, but not always. About 20–30% of children with a successful Kasai procedure can preserve their native liver well into their teens or even adulthood. However, 70–80% will eventually require a liver transplant, typically in the first few years of life. The good news is that paediatric liver transplant outcomes are excellent, with over 90% five-year survival rates.
Can a baby with biliary atresia live a normal life?
Yes. With proper treatment—whether through a successful Kasai procedure or a liver transplant—many children with biliary atresia grow up to attend school, play sports, and lead full, active lives. Worldwide, there are reports of adults who were treated for biliary atresia in infancy going on to hold jobs, attend college, and even become parents themselves.
What should I do if my baby’s jaundice hasn’t cleared by 2 weeks?
See your paediatrician immediately and specifically request a fractionated bilirubin test (which measures direct and indirect bilirubin separately). Also check your baby’s stool colour—photograph it and show it to your doctor. If the direct bilirubin is elevated or stools are pale, your baby should be urgently referred to a paediatric hepatologist or paediatric surgeon for further evaluation. Every day matters.

Keep track of your appointments, get updates & more!

