





Understanding the Role of Rotablators in Treating Calcified Heart Blockages: What Is a Rotablator?
There are various types of blockages in the heart. Some are soft, while others, in older adults or people with conditions such as diabetes, are hard and calcified. Hard blockages in the heart are a challenge to treat. Hard blockages are difficult to treat because they work in a completely different manner from soft plaques. They are unresponsive to balloons, make stents difficult to expand, and increase the risk of failing to open the artery completely during an angioplasty. In such cases, a physician will use a rotablator to prepare the artery for a stent. ¹–³
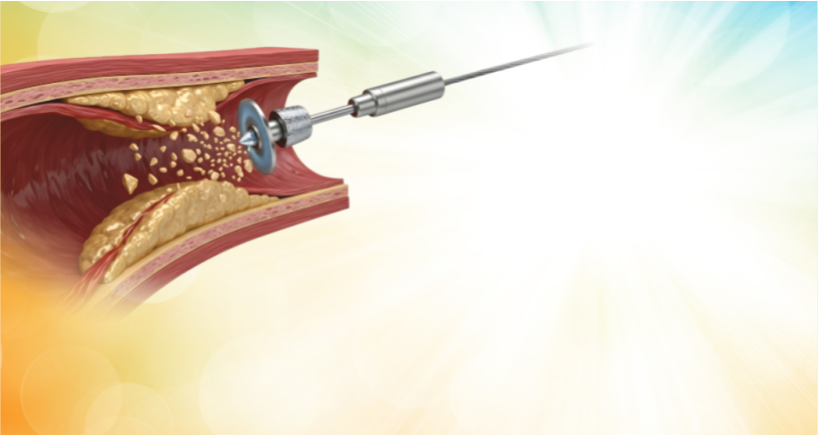
A rotablator is a device used in a heart procedure known as rotational atherectomy. A rotablator is a device used in rotational atherectomy, a heart procedure that carefully sands away hard calcium deposits within the artery. This makes it possible to widen the artery enough to perform an angioplasty. ²
The rotablator features a diamond-coated burr that rotates at high speeds, designed to precisely target and modify calcified blockages. When advanced to the site of a calcified blockage, it grinds the hard calcium while leaving the softer artery tissue largely unaffected. The microscopic calcium particles produced are small enough to pass safely through the bloodstream and be cleared by the body. ¹,³
A rotablator helps by gently smoothing the hard calcium before a stent is placed. This allows the stent to open evenly and fit properly against the artery wall, making the treatment safer and more effective.¹–³
Doctors recommend a rotablation if there's a blockage with a lot of hard calcium, evident from tests like angiography, IVUS, or OCT. These tests help them understand the severity of the blockage and choose the best option.
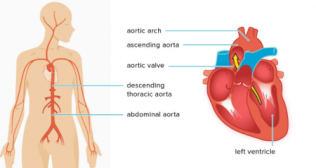
A rotablation is recommended for old blockages, critical arteries like the left main coronary artery, or cases where previous angioplasty failed due to hard plaque. Rather than forcing a stent into an unprepared artery, calcium modification with a rotablator creates a safer foundation for durable results. ³
The rotablator integrates seamlessly into the angioplasty process, playing a crucial role in enhancing the procedure's success by effectively preparing the artery. The procedure is performed through the same arterial access, usually via the wrist or groin, without open surgery. People don't feel the grinding action inside the artery. Recovery is similar to standard angioplasty, guided by the complexity of the overall heart condition rather than the use of the device itself.¹
Safety is a key concern with any advanced intervention, and rotational atherectomy has been extensively studied. When performed by experienced operators in selected individuals, it has a strong safety profile and significantly improves procedural success in calcified lesions. Modern techniques, better imaging guidance, and refined burr designs have further reduced complications compared to earlier years.²,⁴
The rotablator represents a shift in cardiology toward lesion preparation rather than stent deployment. By addressing calcium first, cardiologists can tailor treatment to the blockage's true nature rather than applying a one-size-fits-all approach. This strategy has been shown to reduce repeat procedures and improve long-term outcomes in people with complex coronary artery blockages.³
A rotablator is not a replacement for angioplasty or stenting, but it's a transformative tool that enhances treatment outcomes for patients with calcified heart blockages. For people with hard, calcified heart blockages, it converts a high-risk or incomplete procedure into a precise, controlled, and effective treatment. In advanced coronary care, this small rotating burr often makes a life-saving difference. ¹–³
References
- Barbato E, Shlofmitz E, Milkas A, et al. State of the art: rotational atherectomy. EuroIntervention. 2017;13(6):696–704.
- Abdel-Wahab M, Richardt G, Joachim Büttner H, et al. High-speed rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions. J Am Coll Cardiol. 2013;62(24):2360–2369.
- Räber L, Mintz GS, Koskinas KC, et al. Clinical use of intracoronary imaging. Eur Heart J. 2018;39(35):3281–3300.
- Chambers JW, Behrens AN, Martinsen BJ. Atherectomy devices for the treatment of calcified coronary lesions. Interv Cardiol Clin. 2016;5(2):143–151.
Categories
Clear allMeet the doctor

- Cardiac Sciences | Interventional Cardiology
-
 15 Years
15 Years
-
 1500
1500
Related Blogs
View all







FAQs

Keep track of your appointments, get updates & more!

