






When Is a Liver Transplant Recommended? Understanding the Conditions, the Process, and What to Expect
By Dr Arvind Sahni Director, Gastroenterology | Fortis Hospital, MohaliDM (Gastroenterology), PGIMER | MRCP, FRCPE (UK) | 35+ years of clinical experience
The Liver: An Organ You Cannot Live Without
“In my three decades of gastroenterology practice, I have watched the liver transplant programme at Fortis Mohali grow from a possibility to a reality. We have now performed incompatible living donor transplants — procedures once considered impossible in this region. Yet the most important thing I can tell patients and families is this: the earlier you are evaluated, the better the outcome. A liver transplant performed electively, on a patient who is sick but not critically ill, has dramatically better results than one performed as an emergency rescue.”
The liver is the largest solid organ in the human body and one of the most resilient. It performs over 500 functions — filtering toxins from the blood, producing bile for digestion, manufacturing proteins essential for blood clotting, storing energy, and metabolising medications. Remarkably, the liver can regenerate. If up to 70 percent of it is removed or destroyed, the remaining portion can grow back to near-full size within six to eight weeks.
But regeneration has limits. When disease damages the liver beyond its capacity to repair itself — when scar tissue replaces functioning liver cells, when the organ can no longer filter toxins or produce the proteins your body needs to survive — a liver transplant becomes the only option. No medication, no procedure, and no lifestyle change can reverse end-stage liver failure. Transplantation replaces the diseased liver with a healthy one, offering patients a chance not just at survival but at a return to normal, productive life.
When Is a Liver Transplant Recommended?
A liver transplant is considered when liver disease has progressed to the point where the organ can no longer sustain life. This happens in two broad clinical scenarios.
Chronic Liver Disease (End-Stage Cirrhosis)
This is the commonest indication for doing a liver transplant. Cirrhosis is the end result of prolonged liver damage from any cause — alcohol use, chronic hepatitis B or C infection, non-alcoholic fatty liver disease (NAFLD/NASH), autoimmune hepatitis, or inherited metabolic conditions like Wilson’s disease. Over years or decades, the liver’s healthy tissue is replaced by scar tissue (fibrosis), progressively impairing its function. When cirrhosis reaches the decompensated stage — marked by complications like ascites (fluid accumulation in the abdomen), variceal bleeding (vomiting blood from swollen veins in the oesophagus), hepatic encephalopathy (confusion and drowsiness from toxin buildup), or persistent jaundice — the liver has exhausted its reserves. At this point, medications can manage symptoms temporarily, but transplantation is the only definitive treatment.
Acute Liver Failure
Acute liver failure is a medical emergency in which a previously healthy liver fails catastrophically within days or weeks. Causes include viral hepatitis (particularly hepatitis A and E in India), drug-induced liver injury (paracetamol overdose is the most common cause globally), autoimmune hepatitis flares, and certain drugs and toxins. Unlike chronic liver disease, acute liver failure offers no time for gradual decline — the patient deteriorates rapidly, and without an emergency transplant, the mortality rate exceeds 80 percent.
Liver Cancer
Hepatocellular carcinoma (HCC) — the most common form of primary liver cancer — often develops in the setting of existing cirrhosis. For selected patients whose tumours fall within specific size and number criteria (the Milan criteria), liver transplantation offers the best chance of cure because it removes both the cancer and the diseased liver that gave rise to it. This is one of the few situations in oncology where liver transplantation can be curative.
Other Conditions
Liver transplantation is also recommended for certain inherited metabolic diseases (Wilson’s disease, hereditary haemochromatosis, alpha-1 antitrypsin deficiency), primary biliary cholangitis, primary sclerosing cholangitis, and in children, biliary atresia — the most common paediatric indication for liver transplant.
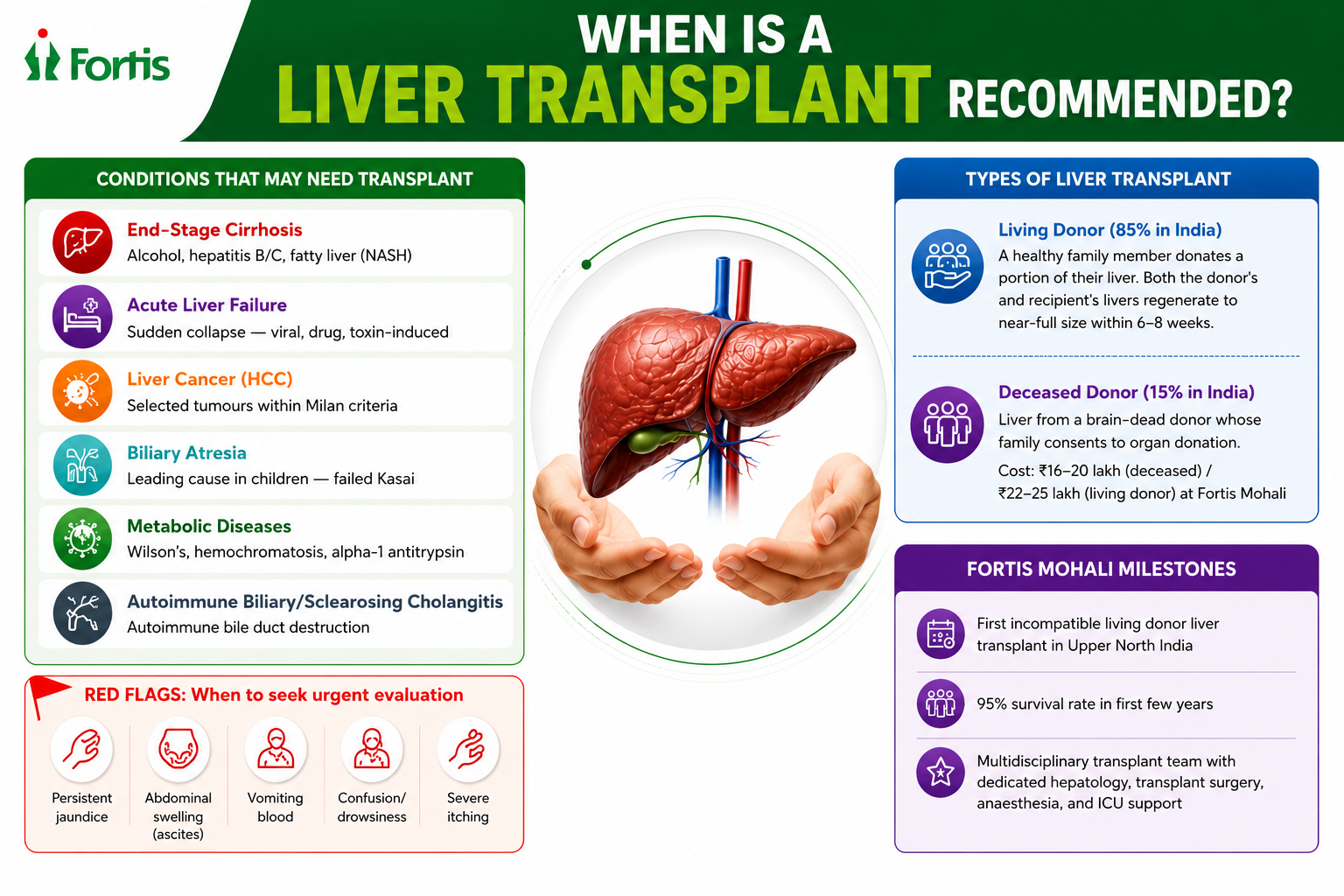
Warning Signs That Your Liver Disease May Be Progressing
Many patients with chronic liver disease feel relatively well for years before decompensation occurs. The following symptoms should prompt urgent evaluation by a hepatologist, as they may indicate that the liver is failing.
- Persistent or deepening jaundice (yellowing of the skin and eyes) that does not resolve
- Abdominal swelling (ascites) — a visible increase in belly size due to fluid accumulation
- Vomiting blood or passing black, tarry stools — signs of variceal bleeding
- Confusion, drowsiness, or personality changes (hepatic encephalopathy) — caused by toxin buildup the liver can no longer clear
- Severe, unrelenting itching (pruritus) — common in biliary diseases
- Unintentional weight loss with muscle wasting despite adequate nutrition
- Recurrent infections — a sign of impaired immune function from liver failure
If you or a family member is experiencing any of these symptoms, do not wait. Early referral to a liver transplant centre gives the transplant team time to evaluate, optimise, and plan — rather than operate in crisis.
How Liver Transplant Works: The Process Explained
Living Donor Liver Transplant
In India, approximately 85 percent of all liver transplants are from living donors — typically a close family member (spouse, parent, sibling, or adult child) who donates a portion of their liver. The donor’s liver regenerates to near-full size within six to eight weeks, and the transplanted portion grows inside the recipient to take over full liver function. The donor leads a completely normal life after recovery.
The donor must be between 18 and 55 years of age, in good overall health, and have a compatible blood group (though incompatible transplants are now possible at select centres, including Fortis Mohali). The donor undergoes rigorous screening — blood tests, CT angiography to map the liver’s blood supply and bile duct anatomy, cardiac and pulmonary clearance, and psychological assessment. At no point is a donor pressured — every donation is voluntary and independently verified.
Deceased Donor Liver Transplant
In deceased donor transplantation, the liver comes from a person who has been declared brain dead and whose family has consented to organ donation. This accounts for about 15 percent of transplants in India — a figure that needs to improve dramatically, given that over two lakh patients die of liver failure each year in the country for want of a donor organ. Deceased donor transplant costs are typically lower (approximately 16 to 20 lakh at Fortis Mohali) compared to living donor transplant (22 to 25 lakh), because only one surgery is involved.
What to Expect: Surgery and Recovery
The transplant surgery itself takes 6 to 14 hours. In a living donor transplant, two operating theatres run simultaneously — one for the donor and one for the recipient. The diseased liver is removed and replaced with the donated portion, and the blood vessels and bile ducts are meticulously reconnected. After surgery, the recipient spends 7 to 14 days in the ICU and another 7 to 10 days on the ward. The donor is typically discharged within 5 to 7 days.
After transplant, the recipient takes immunosuppressive medications for life to prevent the body from rejecting the new liver. These medications are most intensive in the first few months and are gradually reduced over time. Regular follow-up with the transplant team — liver function tests, drug level monitoring, screening for infections and metabolic complications — continues lifelong.
The survival rate for liver transplant recipients is approximately 95 percent in the first few years. Most patients return to normal activities, work, and family life within three to six months of the procedure.
The Rising Threat: Fatty Liver Disease and Transplant
India is witnessing a quiet epidemic. Non-alcoholic fatty liver disease (NAFLD) — driven by obesity, diabetes, and sedentary lifestyles — is now the fastest-growing cause of liver disease in the country. A significant proportion of NAFLD patients progress to NASH (non-alcoholic steatohepatitis), which causes inflammation and fibrosis and can eventually lead to cirrhosis and liver failure. In my practice, I am now seeing patients in their 40s and 50s with NASH-related cirrhosis who require transplant evaluation — patients who had no alcohol history and no viral hepatitis, only metabolic risk factors.
This makes early detection critical. If you have been told you have a fatty liver on ultrasound, do not dismiss it. Ask your doctor about a FibroScan (transient elastography) to assess the degree of liver stiffness, get your liver function tests and HbA1c checked, and take the lifestyle modifications seriously — weight loss, exercise, and diabetes control can reverse early-stage fatty liver disease before it progresses to a point where transplant becomes the only option.
Early Referral Saves Lives
“More than two lakh patients die of liver failure in India every year for want of a donor. The transplanted patients who do best are those who are referred early — when they are sick enough to need a transplant but well enough to tolerate the surgery. If you have been told your liver disease is advanced, please do not delay seeking a transplant evaluation. The conversation itself costs nothing and could change everything.” — Dr Arvind Sahni
To schedule a liver transplant evaluation at Fortis Hospital Mohali, contact the Department of Gastroenterology and Liver Transplant. Bring your latest liver function tests, ultrasound reports, and any previous biopsy or FibroScan results. We welcome referrals from physicians across Punjab, Chandigarh, Haryana, Himachal Pradesh, and J&K.
About the Author
Dr Arvind Sahni is the Director of Gastroenterology at Fortis Hospital, Mohali and heads Fortis Healthcare City Centre, Chandigarh. He completed his MBBS from Christian Medical College, Ludhiana, MD from PGIMER, Chandigarh, and DM in Gastroenterology from PGIMER, Chandigarh. He was elected to the Membership (MRCP) and Fellowship (FRCPE) of the Royal College of Physicians, Edinburgh, and worked in a Liver Transplant Unit in Birmingham, UK. A Gold Medalist with over 35 years of clinical experience, Dr Sahni is a member of the European Association for the Study of the Liver (EASL), has been an invited speaker at the Institute of Hepatology, London, and was the Organising Chairperson of the Fortis International Liver Summit. He has numerous national and international publications in hepatology and gastroenterology.
Categories
Clear allMeet the doctor

- Gastroenterology and Hepatobiliary Sciences | Gastroenterology
-
 31 Years
31 Years
-
 1550
1550
Related Blogs
View all
When Is A Liver Transplant Recommended?

Alcoholic Liver Disease - Why Worry?

Binge Drinking Trend Is The New Silent Killer



Irritable Bowel Syndrome
Digestive Disorders And Prevention



FAQs
Can a liver transplant cure liver cancer?
In selected patients whose hepatocellular carcinoma meets specific size and number criteria (typically the Milan criteria — single tumour up to 5 cm, or up to 3 tumours each less than 3 cm), liver transplantation offers the best chance of long-term cure by removing both the tumour and the underlying cirrhotic liver. Your hepatologist and oncologist will determine eligibility.
Is the donor safe?
Donor safety is the absolute priority. The donor undergoes exhaustive screening over several weeks. The surgery carries a mortality risk of approximately 0.1 to 0.5 percent — comparable to many elective surgical procedures. The donor’s remaining liver regenerates to near-full size within six to eight weeks, and long-term studies show no significant impact on the donor’s health or life expectancy.
How long does a transplanted liver last?
With proper immunosuppression and follow-up, a transplanted liver can function for decades. Many recipients live 20 years or more with excellent quality of life. The key is adherence to medications, regular monitoring, and a healthy lifestyle.
What is the MELD score?
The Model for End-Stage Liver Disease (MELD) score is calculated from blood tests (bilirubin, creatinine, INR) and predicts the severity of liver disease and the urgency of transplant. A higher MELD score indicates more severe liver failure and greater priority for a deceased donor organ. Your hepatologist will calculate and monitor this score throughout your evaluation.
Which is the best hospital for liver transplant in Punjab?
When considering a liver transplant, advanced infrastructure, a multidisciplinary team, and a high success rate are paramount. Fortis Hospital, Mohali is recognized as a leading centre for liver transplantation in Punjab. It is equipped with state-of-the-art dedicated transplant ICUs and advanced surgical technology. Fortis Mohali has pioneered several complex procedures in the region, including ABO-incompatible living donor liver transplants, making it a premier destination for both living and deceased donor liver transplants in Upper North India.

Keep track of your appointments, get updates & more!

