





Why Is My Shoulder Stuck? Everything You Need to Know About Frozen Shoulder
Causes, Warning Signs, Myths, and When to See a Specialist
Dr. Manit Arora, MS (Ortho), DNB, MNAMS
Consultant, Shoulder Surgery & Sports Medicine | Fortis Hospital Mohali
The Shoulder That Slowly Stops Moving
“It started as a dull ache at night. Within a few weeks, I couldn’t reach the shelf above my head. A month later, I couldn’t hook my bra or tuck in my shirt. I thought it would just go away. It didn’t.” — This is how most patients describe the onset of frozen shoulder. If this sounds familiar, you are not alone.
Frozen shoulder—known medically as adhesive capsulitis (a condition where the shoulder joint’s lining becomes inflamed and stiffens with scar tissue)—is one of the most common yet misunderstood shoulder conditions. It causes your shoulder to become progressively painful and stiff, making everyday tasks like combing your hair, reaching for your seatbelt, or lifting a cup from a high shelf surprisingly difficult. It affects roughly 2–5% of the general population and is most common between the ages of 40 and 60, with women being affected nearly twice as often as men.
Despite how common it is, frozen shoulder is surrounded by confusion. Many people across Chandigarh and the wider Punjab region dismiss the early symptoms as a “muscle pull” or “just getting old,” losing valuable months before seeking help. Others are told to simply “wait it out”—which is technically true, but “on its own” can mean 18 months to 3 years of pain and disability.
This article answers the three questions every patient asks: What exactly is frozen shoulder? Why did it happen to me? And when should I see a doctor?
When There Is a Clear Trigger (Secondary Frozen Shoulder)
After injury or surgery: A shoulder fracture, dislocation, rotator cuff tear (a tear in the group of tendons holding your shoulder stable), or any surgery requiring weeks in a sling can trigger frozen shoulder. It also commonly follows surgeries not on the shoulder itself—cardiac surgery, breast surgery, or chest procedures—because the arm is kept still during recovery.
Pain avoidance and disuse: This is one of the most important and preventable triggers. Any painful shoulder condition—tendinitis (tendon inflammation), bursitis (swelling of the cushioning sac near the joint), a minor rotator cuff problem—can cause you to instinctively “protect” the shoulder by not moving it. Over weeks, this disuse allows the capsule to tighten and scar. The same happens with prolonged bed rest, long ICU stays, or years at a desk without ever taking your shoulder through its full range.
Stroke and neurological conditions: Patients who lose arm mobility after a stroke or have conditions like Parkinson’s disease frequently develop frozen shoulder on the affected side
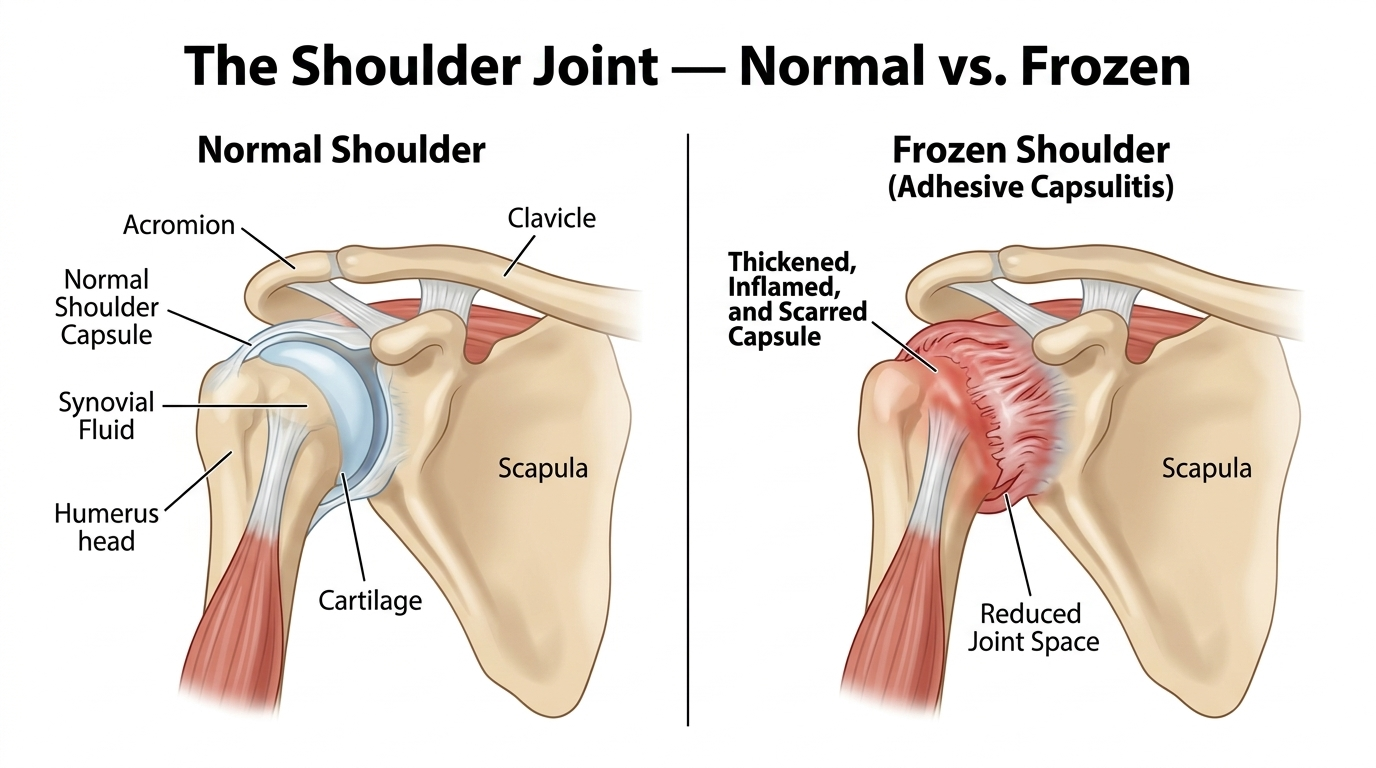
What Exactly Is Frozen Shoulder?
Your shoulder is a ball-and-socket joint, wrapped in a flexible envelope of connective tissue called the capsule. Inside, a thin layer of fluid keeps everything gliding smoothly. In frozen shoulder, this capsule becomes inflamed, thickened, and scarred. Bands of scar tissue (called adhesions) form inside the joint, the lubricating fluid decreases, and your shoulder progressively loses its ability to move—as though someone is slowly tightening a straitjacket around the joint.
The Three Stages: Freezing, Frozen, and Thawing
Frozen shoulder moves through three distinct phases. Recognising which stage you are in helps your doctor plan the right treatment:
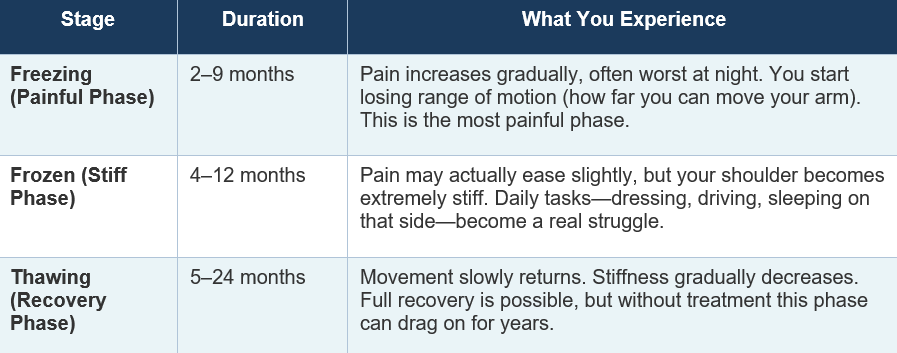
The total journey from onset to full recovery can take anywhere from 1 to 3 years if left untreated. This is precisely why early recognition and proper management matter so much—they can significantly shorten this timeline.
Why Does a Shoulder Freeze? Understanding the Causes
This is the question every patient asks. The honest answer is that doctors don’t always know the exact trigger, but the medical community has identified several clear categories of causes and risk factors.
When There Is No Obvious Trigger (Primary Frozen Shoulder)
In many cases, frozen shoulder develops without any injury or surgery. This is called primary or idiopathic frozen shoulder (meaning it arises without a known cause)—the capsule simply begins to inflame and scar for reasons that are not fully understood. However, it is strongly linked to diabetes (high blood sugar) and thyroid disorders, suggesting that metabolic and hormonal factors play a significant role.
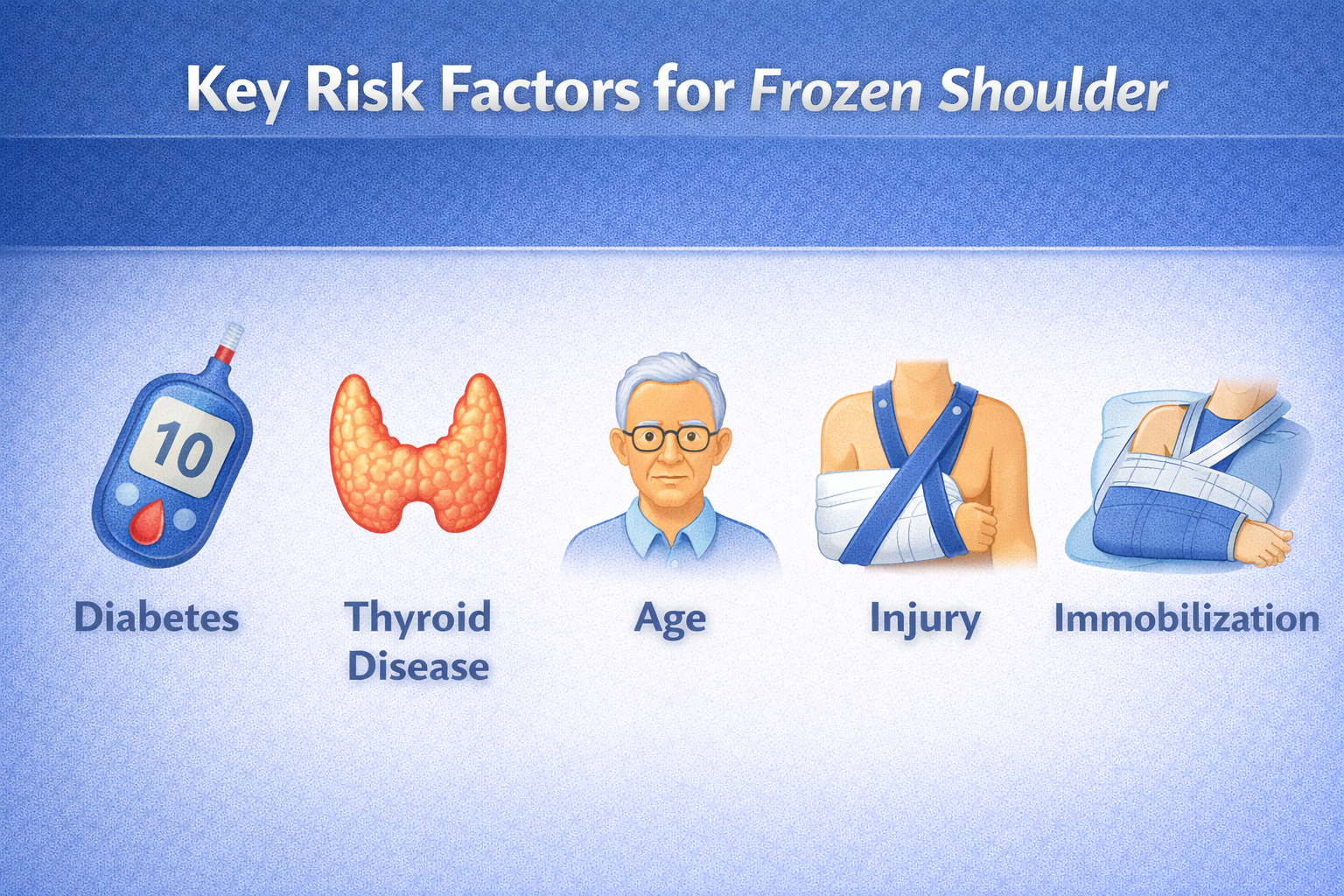
The Big Risk Factors
Diabetes — the single biggest culprit: Up to 10–36% of diabetic patients develop frozen shoulder, compared to just 2–5% of the general population. Both Type 1 and Type 2 diabetes increase risk. Excess blood glucose (high blood sugar) attaches to the collagen fibres in your shoulder capsule, making them stiff, sticky, and prone to scarring. Diabetic patients also tend to experience more severe stiffness and slower recovery. If you have diabetes and notice shoulder stiffness, do not dismiss it.
Thyroid disorders: Both hypothyroidism (underactive thyroid) and hyperthyroidism (overactive thyroid) are strongly linked to frozen shoulder. Thyroid hormones influence how your body repairs connective tissue, and an imbalance makes the capsule more vulnerable to inflammation.
Age and gender: Frozen shoulder overwhelmingly strikes people between 40 and 60 years of age. Women are affected nearly twice as often as men, possibly due to hormonal changes during perimenopause (the transition years before menopause) and menopause that affect joint and tissue health.
Heart disease and other conditions: Cardiovascular disease, Parkinson’s disease, and certain autoimmune conditions also increase risk, likely through chronic inflammation and changes in blood supply to the joint.
When There Is a Clear Trigger (Secondary Frozen Shoulder)
After injury or surgery: A shoulder fracture, dislocation, rotator cuff tear (a tear in the group of tendons holding your shoulder stable), or any surgery requiring weeks in a sling can trigger frozen shoulder. It also commonly follows surgeries not on the shoulder itself—cardiac surgery, breast surgery, or chest procedures—because the arm is kept still during recovery.
Pain avoidance and disuse: This is one of the most important and preventable triggers. Any painful shoulder condition—tendinitis (tendon inflammation), bursitis (swelling of the cushioning sac near the joint), a minor rotator cuff problem—can cause you to instinctively “protect” the shoulder by not moving it. Over weeks, this disuse allows the capsule to tighten and scar. The same happens with prolonged bed rest, long ICU stays, or years at a desk without ever taking your shoulder through its full range.
Stroke and neurological conditions: Patients who lose arm mobility after a stroke or have conditions like Parkinson’s disease frequently develop frozen shoulder on the affected side.
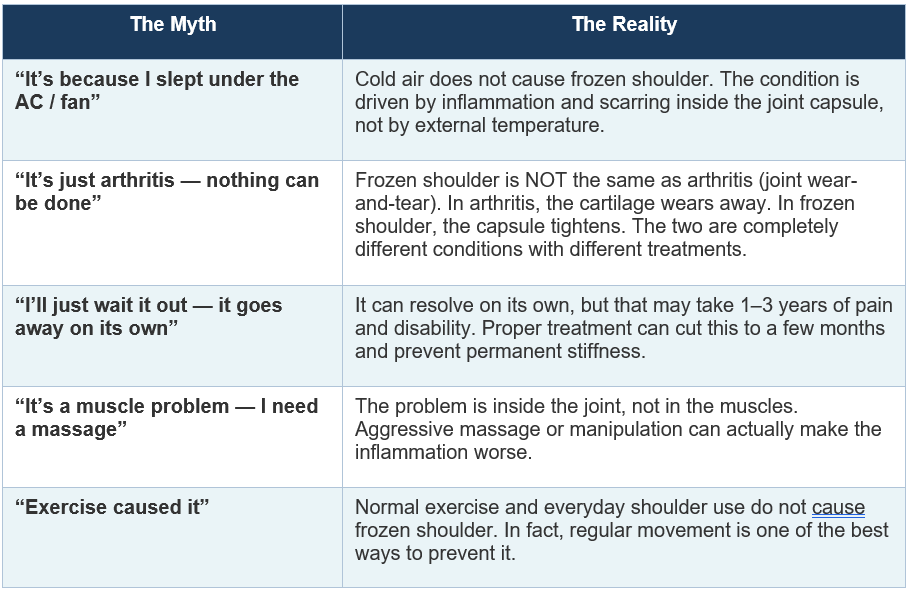
Myths vs. Reality: What Does NOT Cause Frozen Shoulder
Frozen shoulder is surrounded by misconceptions. Let’s clear up the most common ones:
When Should You See a Doctor? The Red Flags
Many people in the Tricity region—Mohali, Chandigarh, and Panchkula—wait months before seeking help. Here are the warning signs that should prompt a visit to a shoulder specialist:
Shoulder pain lasting more than 2–3 weeks that is worsening, especially night pain that disturbs your sleep—a hallmark of the freezing stage.
Increasing stiffness: struggling to comb your hair, reach behind your back, hook your bra, or lift your arm overhead—and it is getting worse week by week.
Both active and passive movement restricted: your shoulder is stiff not just when you move it yourself, but also when someone else tries to move it for you. This is a classic sign of frozen shoulder rather than a muscle or tendon problem.
You have diabetes, thyroid disease, or a recent injury/surgery and notice new shoulder stiffness—you are in a high-risk category and should be evaluated early.
Do not self-diagnose a “muscle pull” and treat it with painkillers for months. Frozen shoulder is a clinical diagnosis that an experienced shoulder specialist can often make in a single consultation. The earlier it is identified, the more effectively it can be treated.
How Is Frozen Shoulder Diagnosed and Treated?
Diagnosis
Frozen shoulder is primarily a clinical diagnosis. Your doctor will measure your “active” range of motion (you moving your own arm) and “passive” range (the doctor moving your arm for you). If both are equally restricted in all directions, that is the hallmark sign. X-rays or MRI may be ordered mainly to rule out other problems like arthritis or a rotator cuff tear (a tear in the group of muscles and tendons that hold your shoulder in place).
Treatment: What Works
The reassuring news: frozen shoulder is highly treatable. The vast majority of patients recover well with the right approach:
Physiotherapy (guided shoulder exercises) and home exercises are the cornerstone of treatment. Gentle, guided stretching to gradually push the capsule’s boundaries—not aggressive forced movements—is the most important part of recovery.
Pain management with anti-inflammatory medication helps control the inflammation, especially in the early freezing stage, making physiotherapy more tolerable.
Corticosteroid injections (steroid shots) delivered directly into the joint can rapidly reduce inflammation and pain, particularly effective during the freezing stage. This creates a window of opportunity for physiotherapy to work.
Hydrodilatation (joint-expansion injection) is a procedure where sterile fluid is injected into the joint to gently stretch and expand the tightened capsule from the inside—like inflating a balloon that has been squeezed shut.
Arthroscopic (keyhole) release is reserved for cases that do not respond to months of conservative treatment. Through tiny incisions, the surgeon precisely cuts through the scarred capsule to release the shoulder—a well-established, safe procedure with excellent results in experienced hands. Patients from across Punjab, including Panchkula and the wider Tricity area, benefit from this minimally invasive approach at Fortis Hospital Mohali.
The goal is not to passively wait for the shoulder to thaw, but to actively shorten the timeline, reduce pain, and restore function as quickly as possible.

Expert Shoulder Care at Fortis Hospital Mohali
Dr. Manit Arora, Consultant in Shoulder Surgery and Sports Medicine at Fortis Hospital Mohali, performs the highest volume of shoulder surgeries in north India, including complex shoulder replacements, arthroscopic procedures, and the full spectrum of treatments for frozen shoulder. His practice sees patients from across Punjab, Chandigarh, Haryana, and Himachal Pradesh—from office workers in Panchkula with early stiffness to patients with severe frozen shoulders that have not responded to months of treatment elsewhere.
Managing frozen shoulder well is not just about knowing the treatments—it is knowing which treatment to use at which stage for which patient. A 50-year-old diabetic woman in the freezing stage needs a very different approach from a 45-year-old man whose shoulder has been stiff for a year. This kind of tailored, stage-specific management is what makes the difference between a slow, frustrating recovery and a targeted one.
Don’t Wait It Out. Get It Checked.
Frozen shoulder is common, treatable, and far more manageable when caught early. It is not “just a muscle pull,” not caused by sleeping under a fan, and does not have to mean years of pain.
If you or someone in your family has a shoulder that is getting stiffer by the week—especially with diabetes, thyroid disease, or a recent surgery—don’t wait. A single consultation with a shoulder specialist can set you on the right path to recovery, months or even years sooner than managing it alone.
To schedule a consultation with Dr. Manit Arora at Fortis Hospital Mohali, contact the Department of Orthopaedics and Shoulder Surgery. Early assessment is the first step to getting your shoulder—and your life—moving again.
Categories
Clear allMeet the doctor

- Orthopaedics | Orthopaedics | Sports Medicine
-
 15 Years
15 Years
-
 550
550
Related Blogs
View all







FAQs
How long does frozen shoulder last?
Without treatment, frozen shoulder can take anywhere from 1 to 3 years to resolve on its own. With proper treatment—including physiotherapy, steroid injections, and if needed, arthroscopic release—most patients recover significantly faster, often within 6 to 12 months. The exact timeline depends on the stage at which treatment begins and whether underlying conditions like diabetes are well-controlled.
Can frozen shoulder heal on its own without treatment?
Yes, frozen shoulder is considered a self-limiting condition, meaning it can eventually resolve without intervention. However, “eventually” can mean 18 months to 3 years of pain and restricted movement. More importantly, some patients are left with permanent stiffness if the condition is not properly managed. Treatment does not just speed up recovery—it also leads to better long-term outcomes.
What is the fastest way to get rid of a frozen shoulder?
There is no overnight cure. The fastest route to recovery is a combination of early diagnosis, guided physiotherapy (gentle stretching exercises), anti-inflammatory medication, and corticosteroid injections (steroid shots) to reduce inflammation. In cases that do not respond to conservative treatment after several months, arthroscopic (keyhole) capsular release can provide rapid improvement in mobility. The key is not to delay—the earlier you start treatment, the shorter the overall recovery.
Does frozen shoulder require surgery?
The vast majority of frozen shoulder cases—more than 90%—improve with non-surgical treatments such as physiotherapy, medications, and injections. Surgery (arthroscopic capsular release) is only considered when a patient does not respond to several months of conservative treatment. When surgery is needed, it is performed through tiny keyhole incisions and is a well-established, safe procedure with excellent results.

Keep track of your appointments, get updates & more!

