





Beyond the Pain: When Is a Hysterectomy Medically Necessary? A Gynaecologist’s Guide to Understanding the Decision
Understanding Hysterectomy: It’s Not the First Step
“Hearing the word ‘hysterectomy’ can feel overwhelming. But I want every woman to know: this is never my first recommendation. It is a carefully considered decision we arrive at together, when your quality of life is severely compromised or your health is at risk.” — Dr. Swapna Misra
A hysterectomy is the surgical removal of the uterus. It is one of the most common gynaecological surgeries performed worldwide, yet it remains one of the most emotionally charged. For many women, the uterus carries deep personal and cultural significance, and the prospect of its removal can trigger anxiety, grief, or confusion. These feelings are entirely valid, and they deserve to be heard and addressed before any surgical decision is made.
At its core, a hysterectomy is a treatment, not a diagnosis. It may be performed through several approaches—traditional open abdominal surgery, vaginal hysterectomy, laparoscopic (keyhole) surgery, or the most advanced option available today, robotic-assisted hysterectomy using the da Vinci Xi Surgical System, the globally recognised gold standard in robotic surgery—each offering different trade-offs in terms of recovery, precision, and suitability. Critically, modern gynaecological practice demands that hysterectomy be considered only after conservative treatments have been exhausted or are clearly inappropriate, especially for benign (non-cancerous) conditions.
Recognising the Warning Signs: When Should You Seek Evaluation?
Not every symptom requires surgery. But certain persistent or worsening signs should prompt you to consult a gynaecologist for thorough evaluation. Think of these as signals that your body is asking for help:
Heavy or irregular menstrual bleeding that soaks through pads or tampons every hour, lasts longer than seven days, or has led to iron-deficiency anaemia. If your periods are dictating your schedule—causing you to miss work, avoid social engagements, or live in constant worry—this warrants investigation.
Chronic pelvic pain that persists beyond the menstrual cycle and does not respond to initial medical management, including painkillers and hormonal therapy. Pain that disrupts sleep, intimacy, or daily functioning is not something you should simply endure.
Pressure symptoms—a feeling of heaviness in the lower abdomen, frequent urination, difficulty emptying the bladder, constipation, or visible abdominal distension. These often point to fibroids or an enlarged uterus pressing on surrounding organs.
A bulge or dragging sensation in the vagina, especially when standing, walking, or straining. This is the hallmark of uterine prolapse and should not be dismissed as a normal part of ageing.
If any of these describe your experience, the first step is not surgery—it is a proper diagnosis. But ignoring them can allow the underlying condition to worsen.
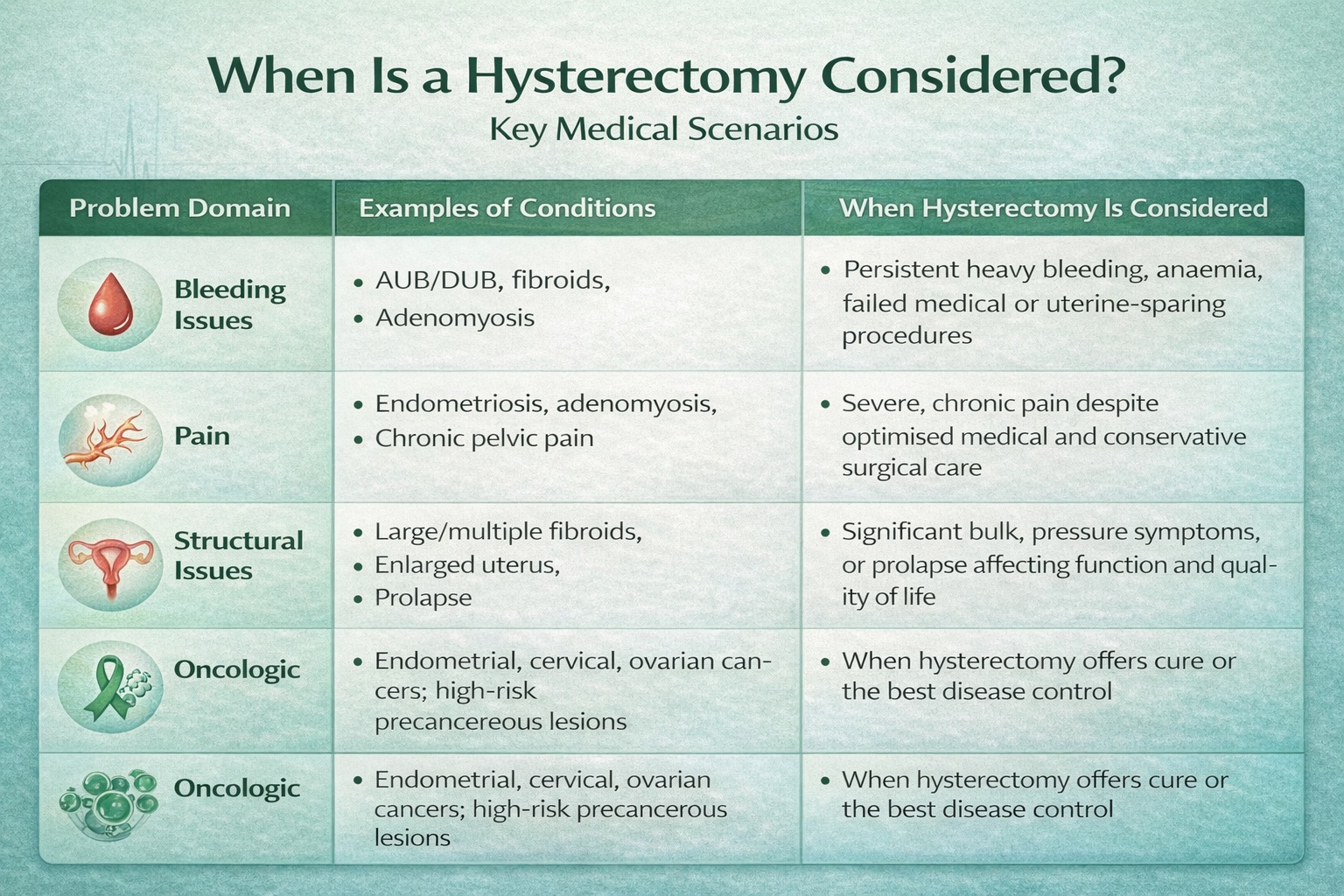
The Five Most Common Reasons a Hysterectomy May Be Considered
The decision to recommend a hysterectomy is never taken lightly. It depends on the specific diagnosis, the severity of your symptoms, your age, whether you wish to have children in the future, and how you have responded to prior treatments. Here are the principal conditions where hysterectomy enters the conversation:
1. Uterine Fibroids
Fibroids are non-cancerous growths that develop in or on the uterus. They are extraordinarily common—affecting up to 70–80% of women by the age of 50—but most are small and symptom-free. The problem arises when fibroids grow large, multiply, or position themselves in ways that cause debilitating pelvic pain, dangerously heavy bleeding, severe anaemia, urinary frequency, or an enlarged abdomen. When fibroids are too large or numerous for a myomectomy (surgical removal of fibroids while preserving the uterus) or when they recur after prior treatment, hysterectomy provides a definitive solution.
2. Adenomyosis and Abnormal Uterine Bleeding
Adenomyosis occurs when the tissue that normally lines the uterus grows into the muscular wall, causing the uterus to enlarge and triggering severe menstrual cramps, heavy bleeding, and chronic pain. Similarly, abnormal uterine bleeding (sometimes called dysfunctional uterine bleeding or DUB) can stem from hormonal imbalances, endometrial hyperplasia, or structural issues. When these conditions cause persistent heavy bleeding that leads to anaemia and significantly impairs quality of life—and when medications, hormonal IUDs like the levonorgestrel intrauterine system, endometrial ablation, and other uterine-sparing procedures have been tried without success—hysterectomy may be the next appropriate step.
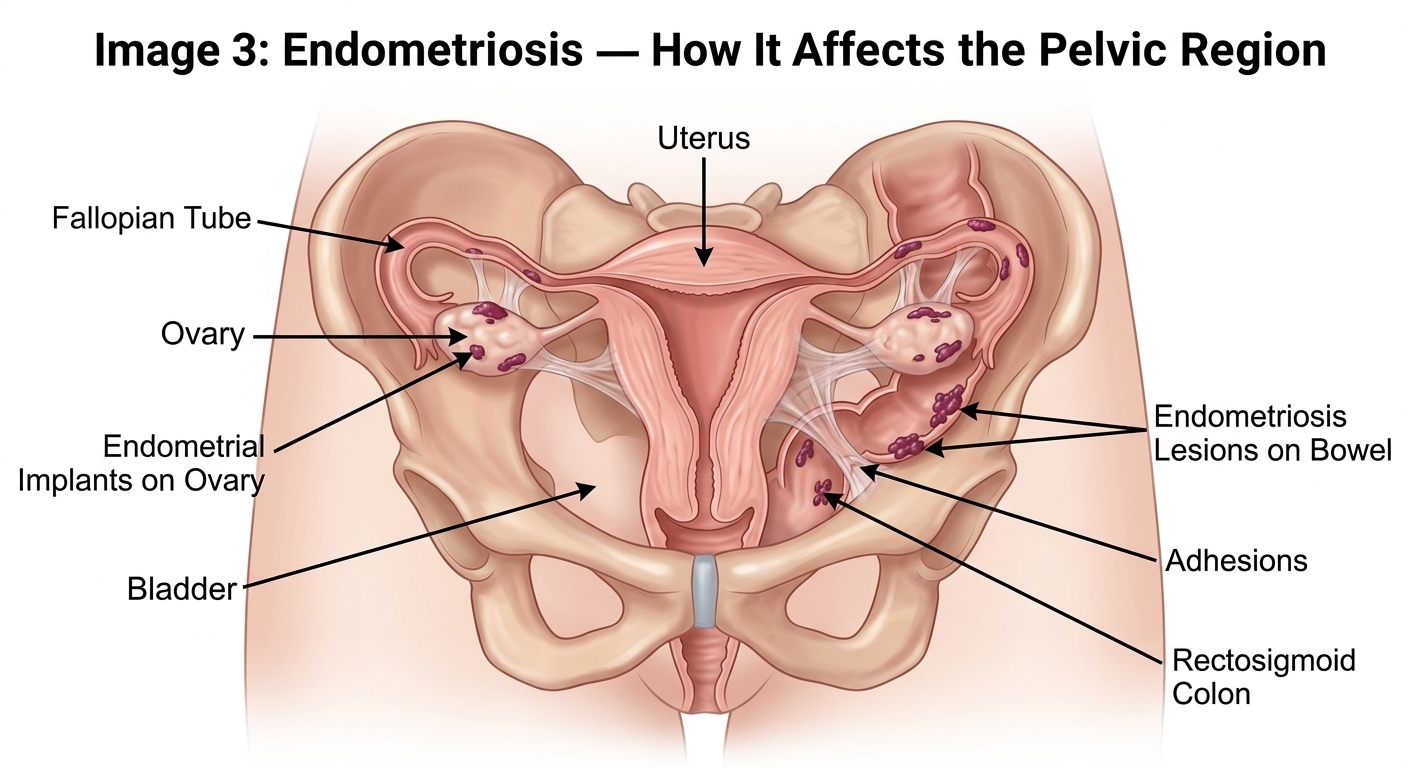
3. Endometriosis
In endometriosis, tissue similar to the uterine lining grows outside the uterus—on the ovaries, fallopian tubes, bowel, or pelvic lining. It can cause chronic pelvic pain, agonising periods, pain during intercourse, and infertility. Many women live with endometriosis for years, managed with hormonal therapy and conservative laparoscopic excision of lesions. However, in severe, deeply infiltrating endometriosis that is resistant to medical and conservative surgical treatment, a hysterectomy—sometimes combined with removal of the affected tissue and ovaries—may offer the best chance of lasting relief.
4. Uterine Prolapse
Uterine prolapse occurs when the pelvic floor muscles weaken and the uterus descends into or beyond the vaginal canal. It is commonly associated with multiple childbirths, ageing, chronic straining, and obesity. Symptoms include a dragging sensation, difficulty with urination or bowel movements, discomfort during walking or sitting, and impaired sexual function. While mild prolapse may respond to pelvic floor exercises (Kegel exercises) or pessary devices, significant prolapse that substantially affects bladder, bowel, sexual function, or daily activities often requires surgical correction, including hysterectomy.
5. Gynaecological Cancers and High-Risk Precancerous Conditions
For cancers of the uterus (endometrial cancer), cervix, or ovaries, hysterectomy is frequently a non-negotiable, life-saving procedure. It may also be recommended for high-risk precancerous conditions such as endometrial hyperplasia with atypia, where the risk of progression to cancer is significant. In these situations, the decision is not about quality of life alone—it is about survival. The type and extent of hysterectomy (total, radical, or with removal of ovaries and lymph nodes) depends on the cancer type, stage, and individual patient factors.
The Tipping Point: A Patient’s Journey
Consider Meera (name changed), a 45-year-old teacher from Chandigarh. For five years, she suffered heavy periods that worsened with every cycle. She tried hormonal tablets, a Mirena IUD, and even underwent endometrial ablation. Each provided temporary relief before the bleeding returned, heavier than before. Diagnosed with adenomyosis and multiple fibroids, she was severely anaemic, exhausted, and had stopped attending school events she once loved. After a detailed discussion weighing all options, she and her gynaecologist decided together that a hysterectomy was the right path forward.
This is the reality for many women: hysterectomy is not a snap decision. It is the culmination of a journey—often years long—through diagnosis, medical management, and careful shared decision-making. The tipping point comes when the condition’s impact on your life outweighs the desire to preserve the uterus.
Hysterectomy Is Not the First Step: The Importance of Exhausting Alternatives
Before recommending hysterectomy for any benign condition, a responsible gynaecologist will ensure that appropriate alternatives have been explored:
Medical management: Hormonal medications, tranexamic acid for heavy bleeding, pain management protocols, and the levonorgestrel intrauterine system (Mirena) for abnormal bleeding and adenomyosis.
Uterine-sparing procedures: Myomectomy for fibroids, endometrial ablation, uterine artery embolisation, and laparoscopic excision of endometriosis.
Imaging and biopsy: Proper evaluation with ultrasound, MRI, and endometrial biopsy where indicated to confirm the diagnosis before proceeding.
Equally important is the shared decision-making conversation. Your age, desire for future pregnancy, overall health, personal preferences, and a clear understanding of the risks and benefits must all factor into the decision. No two women are the same, and the treatment plan should reflect your individual circumstances.
Acknowledging the Emotional Side
It would be incomplete to discuss hysterectomy without acknowledging its emotional dimension. For many women, particularly younger women or those who had hoped to conceive, the loss of the uterus can trigger feelings of grief, a sense of altered identity, or anxiety about intimacy and femininity. These feelings are normal and should be discussed openly with your medical team. Counselling support, both before and after surgery, can be invaluable. A good gynaecologist does not just treat the condition—she treats the whole woman.
A Message of Hope: Modern Surgery Has Changed Everything
If, after careful evaluation, a hysterectomy is determined to be the right path for you, there is genuinely good news: the surgical experience has been transformed. It is no longer the painful, weeks-long recovery of the past. Today, minimally invasive approaches—particularly robotic-assisted hysterectomy—offer smaller incisions (as tiny as 5–8 mm), dramatically less blood loss, significantly reduced pain, hospital stays as short as one day, and a return to normal activities within one to two weeks instead of six.
Once hysterectomy is indicated, the choice of surgical route—vaginal, laparoscopic, robotic, or open abdominal—is tailored to your anatomy, the size and nature of the pathology, any history of prior surgeries, and your surgeon’s expertise. For complex cases—large fibroids, dense adhesions from endometriosis, obesity, or cancer staging—robotic surgery offers a level of precision, 3D visualisation, and instrument dexterity that exceeds what the human hand can achieve through conventional laparoscopy.

Why the da Vinci Xi Matters: Not All Robotic Systems Are Equal
With the growing popularity of robotic surgery, several newer robotic platforms have entered the market. However, it is important for patients to understand that not all robotic systems offer the same capabilities, safety record, or clinical evidence. The da Vinci Xi Surgical System by Intuitive remains the most extensively validated robotic platform in the world, backed by over two decades of clinical use, millions of procedures across 67 countries, and the largest body of peer-reviewed evidence of any surgical robot. Its distinguishing features include:
True wristed instrumentation with 7 degrees of freedom — the EndoWrist instruments replicate the dexterity of the human wrist inside the body, enabling suturing, dissection, and tissue handling with a precision that rigid-instrument systems simply cannot match.
Immersive 3D HD magnified vision — the surgeon operates with up to 10x magnification and stereoscopic depth perception, critical for identifying delicate structures like ureters and blood vessels in the pelvis.
Integrated fluorescence imaging (Firefly) — allows real-time visualisation of blood flow and tissue perfusion during surgery, a capability absent in most competing platforms.
Tremor filtration and motion scaling — the system filters out natural hand tremor and allows the surgeon to scale down movements for ultra-fine manoeuvres in confined spaces.
Multi-quadrant access and overhead boom architecture — unique to the Xi model, allowing the robotic arms to be repositioned for multi-quadrant surgery without re-docking, essential for complex procedures involving the pelvis, abdomen, and retroperitoneum.
Newer, less-established robotic platforms may offer lower acquisition costs, but they often lack the extensive clinical validation, the breadth of instrument options, the proven safety track record, and the surgeon training ecosystem that the da Vinci platform provides. When it comes to a procedure as significant as hysterectomy, patients deserve the platform with the most proven outcomes—and that is the da Vinci Xi.

At Fortis Hospital Mohali, Dr. Swapna Misra—Director of Robotic and Laparoscopic Gynaecology Surgery with over 20,000 surgical procedures to her credit—leads one of north India’s most advanced robotic gynaecology programmes. Operating on the da Vinci Xi Surgical System, her team routinely performs complex hysterectomies with outcomes that include minimal blood loss, near-zero major complication rates, and the vast majority of patients returning home within 24 hours. Fortis Mohali’s commitment to the da Vinci Xi platform reflects its philosophy of offering patients the most clinically validated technology available—not the newest marketing claim, but the most proven surgical system in the world.
“The da Vinci Xi is not just a robot—it is an extension of the surgeon’s hands and eyes, inside the patient’s body. It empowers us to perform the most complex procedures with a precision and gentleness that transforms the surgical experience for women.” — Dr. Swapna Misra
Conclusion
Hysterectomy is an important treatment for several serious gynaecological conditions—from fibroids and endometriosis to uterine prolapse and gynaecological cancers. But it should never be a hasty decision. It should follow thorough evaluation, exhaustion of appropriate alternatives, and a collaborative conversation between you and your gynaecologist that respects your medical needs, your emotional well-being, and your life goals.
The advances in surgical technology—particularly robotic hysterectomy on the da Vinci Xi platform—mean that when surgery is necessary, it can be performed with a precision, safety, and speed of recovery that would have been unimaginable a generation ago. In our next article, Dr. Swapna Misra explains exactly how robotic hysterectomy with the da Vinci Xi works, who it is ideal for, and why Fortis Hospital Mohali has become a destination for women seeking the most advanced gynaecological care in the region.
To learn more about your treatment options or to schedule a consultation with Dr. Swapna Misra at Fortis Hospital Mohali, contact the Department of Gynaecology today.
Contact Us – Fortis Hospital Mohali
For appointments, consultations, and diagnostic services, please contact:
📞 72728 72728
Our care team will assist you with:
Doctor appointments
Diagnostic and screening services
Health check-ups
Call now to book your appointment at Fortis Hospital, Mohali.
Categories
Clear allMeet the doctor

- Oncology | Surgical Oncology
- Obstetrics and Gynaecology | Gynaecologic Oncology | Obstetrics and Gynaecology
-
 23 Years
23 Years
-
 1250
1250
Related Blogs
View all

Bacterial Vaginosis: Causes, Symptoms And Treatment


Awareness, Breast Self-Examination And Regular Screening Examination Can Change The Life o...

Hormonal Imbalance: Symptoms, Causes And Treatment

Evolution of Gynae & Cancer Surgeries With Robotics


Know The Top 11 Benefits of Antenatal Exercises


FAQs

Keep track of your appointments, get updates & more!

