






Breast Cancer Treatment Options: From Breast-Conserving Surgery to Robotic Nipple-Sparing Mastectomy
By Dr Deepti Singh Consultant, Breast Surgery & Surgical Oncology | Fortis Cancer Institute, Mohali
A Diagnosis Is Not the End — It Is the Beginning of a Plan
There is no single treatment for breast cancer. Every treatment plan is tailored to the individual patient — her cancer type, stage, biology, genetics, age, overall health, and personal goals. The purpose of this guide is to walk you through every major treatment option, including the latest advances in robotic surgery, so that you can enter the conversation with your oncology team informed and empowered.
If you have recently been diagnosed with breast cancer, you are likely overwhelmed by terminology, decisions, and fear. That is completely understandable. But breast cancer treatment has evolved dramatically. Today, many women achieve excellent cancer outcomes while preserving their body image, breast sensation, and quality of life. The key is understanding your options — and this blog exists to give you that understanding.
Your Treatment Journey: From Diagnosis to Survivorship

At Fortis Cancer Institute Mohali, every breast cancer patient’s case is reviewed by a multidisciplinary tumour board: surgical oncologist, medical oncologist, radiation oncologist, radiologist, and pathologist. This team approach ensures that treatment decisions are based on the full clinical picture — tumour stage, receptor status (ER/PR, HER2), BRCA mutation status, imaging findings, and the patient’s own priorities.
Surgery: The Foundation of Breast Cancer Treatment
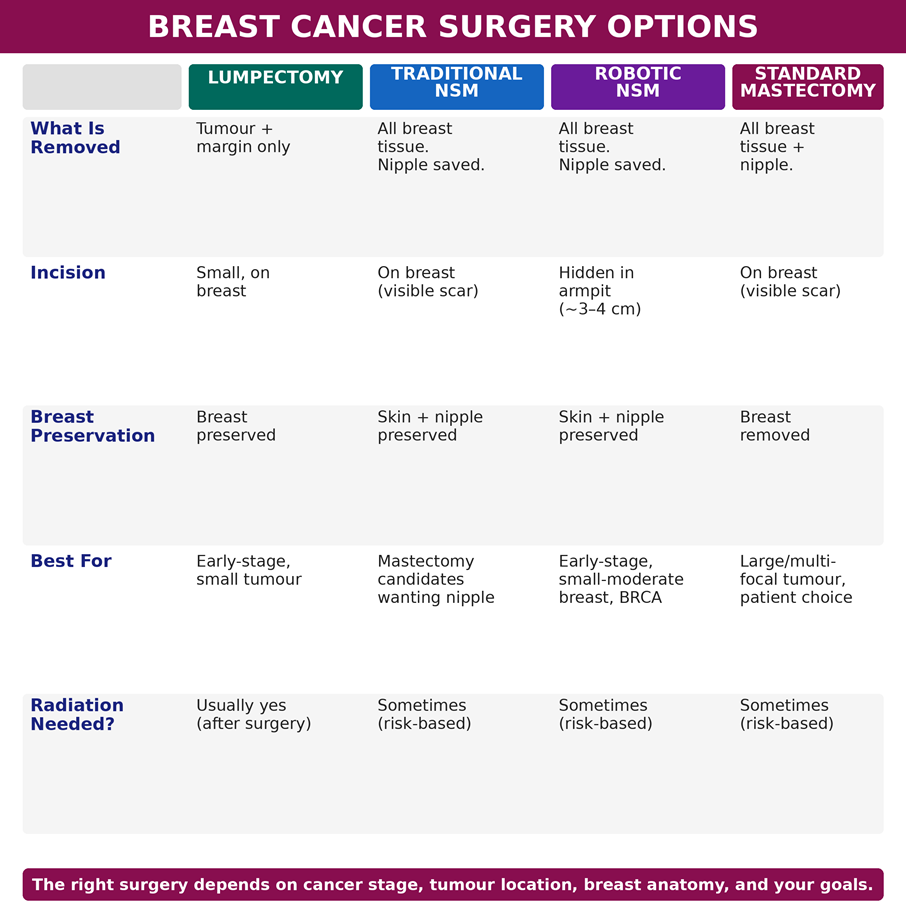
Breast-Conserving Surgery (Lumpectomy)
Lumpectomy removes the tumour with a margin of healthy tissue while preserving most of the breast. It is usually followed by radiation therapy. For many early-stage breast cancers, lumpectomy plus radiation achieves survival outcomes comparable to mastectomy (NCCN Guidelines, EBCTCG meta-analysis). It remains the preferred option whenever oncologically safe and anatomically feasible.
Mastectomy: When More Tissue Needs to Come Out
Mastectomy — removal of the entire breast — is recommended when the tumour is large, multifocal (multiple tumours), when the patient carries a BRCA1/BRCA2 mutation, when prior radiation has been received, or when the patient herself prefers it. Modern mastectomy has evolved far beyond the radical procedures of the past.
Nipple-Sparing Mastectomy (NSM)
In carefully selected patients, the breast tissue is removed while the skin envelope and nipple-areola complex are preserved — allowing immediate reconstruction with dramatically better cosmetic outcomes and psychological recovery. The critical requirement: the tumour must be located a safe distance from the nipple, with no evidence of nipple involvement on imaging or frozen section.
Robotic Nipple-Sparing Mastectomy: The Next Evolution
Robotic nipple-sparing mastectomy (RNSM) adds the precision of the da Vinci robotic platform to an already advanced surgical concept. The surgeon operates from a console, using 3D high-definition magnified vision and wristed robotic instruments inserted through a single small incision hidden in the armpit (~3–4 cm). The entire breast tissue is removed through this hidden incision, preserving the skin, nipple, and areola for immediate reconstruction.
Why Robotic Matters
- Hidden scar — no visible incision on the breast itself. The scar is concealed in the axillary fold
- Superior visualisation — 10× magnified 3D view allows precise dissection around the nipple-areola complex, protecting blood supply and nerve pathways
- Lower nipple necrosis — published data shows 0% nipple ischaemia in robotic groups versus 2.7% in conventional NSM (meta-analysis, BMC Surgery)
- Fewer major complications — relative risk 0.44 for Grade III+ complications compared with conventional NSM
- Sensation preservation — up to 80% of patients report retained nipple/skin sensation in select studies, compared with variable rates in traditional approaches
- Comparable oncological safety — recurrence rates of 3.8% (robotic) versus 5.9% (conventional) at median follow-up, with no compromise in cancer outcomes
While surgeons focus on removing the cancer, patients are also deeply concerned about losing their physical identity, breast sensation, and dealing with extensive scarring. Robotic NSM addresses all three concerns without compromising cancer safety. But it is not suitable for every patient.
Who Is a Candidate for Robotic Nipple-Sparing Mastectomy?
RNSM is not a one-size-fits-all procedure. International consensus panels (Ryu et al., 2023) have established clear criteria:
- Early-stage breast cancer (Stage 0, I, or II) with tumour size ≤ 5 cm
- Tumour located a safe distance from the nipple (≥ 5 mm on MRI) with no nipple-areola involvement
- Small to moderate breast size (generally C-cup or smaller) — because robotic instruments must reach across the chest from the armpit
- Minimal breast ptosis (sagging) — severe drooping makes robotic access difficult and cosmetic outcomes less predictable
- Non-smoker — nicotine constricts blood vessels and increases nipple necrosis risk. Complete cessation required before and after surgery
- No prior chest radiation — radiation changes tissue quality and blood supply
- BRCA1/BRCA2 carriers undergoing prophylactic (risk-reducing) mastectomy — an excellent application where there is no active cancer
When RNSM is NOT appropriate: inflammatory breast cancer, tumour directly beneath or invading the nipple, T4 lesions with skin involvement, chest wall invasion, or large/very ptotic breasts where cosmetic outcomes would be suboptimal.
Breast Reconstruction After Cancer Surgery
Immediate reconstruction: Performed during the same operation as the mastectomy. Implant-based or autologous tissue (DIEP flap, TRAM flap). Robotic NSM pairs particularly well with immediate implant reconstruction because the preserved skin envelope and nipple provide a natural-looking result from day one.
Delayed reconstruction: Performed weeks to months later, allowing time for adjuvant treatments. Appropriate when radiation therapy is planned post-mastectomy.
Beyond Surgery: Systemic Treatments
Chemotherapy
May be given before surgery (neoadjuvant) to shrink the tumour and enable breast conservation, or after surgery (adjuvant) to eliminate microscopic residual disease. The decision depends on tumour size, lymph node involvement, grade, and molecular subtype.
Hormone Therapy
For hormone receptor-positive (ER/PR+) cancers — the most common subtype. Tamoxifen (premenopausal) or aromatase inhibitors (postmenopausal) block the hormonal fuel that drives these cancers. Treatment typically continues for 5–10 years and significantly reduces recurrence.
Targeted Therapy
For HER2-positive cancers: trastuzumab (Herceptin), pertuzumab, and newer antibody-drug conjugates (ADCs) like trastuzumab deruxtecan (T-DXd). CDK4/6 inhibitors (ribociclib, palbociclib) for hormone-positive advanced disease. PARP inhibitors for BRCA-mutated cancers. These precision treatments target the specific molecular drivers of the cancer.
Immunotherapy
For triple-negative breast cancer (TNBC): checkpoint inhibitors such as pembrolizumab, combined with chemotherapy, are now standard in eligible patients — representing a major advance for a subtype that previously had fewer targeted options.
Radiation Therapy
Typically recommended after lumpectomy to reduce local recurrence. May also be used after mastectomy in higher-risk cases (large tumour, positive lymph nodes, close margins). Modern techniques including hypofractionated schedules have shortened treatment courses from 5–6 weeks to 3–4 weeks or less.
If you have been diagnosed with breast cancer, a consultation with a breast surgical oncologist can help determine whether breast-conserving surgery, nipple-sparing mastectomy, robotic surgery, or another treatment approach is most appropriate for your specific diagnosis. Schedule a multidisciplinary evaluation at the Fortis Cancer Institute, Mohali, with Dr Deepti Singh and the breast cancer team.
About the Author
Dr Deepti Singh is a Consultant in Breast Surgery and Surgical Oncology at Fortis Cancer Institute, Mohali. She specialises in breast cancer surgery, including breast-conserving surgery, nipple-sparing mastectomy, robotic breast surgery, oncoplastic techniques, and sentinel lymph node biopsy. Dr Singh works within the multidisciplinary breast cancer programme at Fortis Mohali, collaborating with medical oncology, radiation oncology, radiology, pathology, plastic surgery, and genetic counselling to deliver personalised, evidence-based cancer care.
Categories
Clear allMeet the doctor

- General Surgery | General and Laparoscopic Surgery
- Endocrine Surgery | Breast and Endocrine Surgery
-
 5 Years
5 Years
-
 950
950
Related Blogs
View all



FAQs
Is lumpectomy always safer than mastectomy?
Lumpectomy is not “safer” in terms of cancer outcomes — survival rates are comparable for early-stage cancers when lumpectomy is combined with radiation. The choice depends on tumour characteristics, genetics, and personal preference.
Will preserving the nipple increase my cancer risk?
When patient selection criteria are followed (adequate tumour-nipple distance, negative frozen section), nipple-sparing mastectomy does not increase cancer recurrence risk. Published data confirms comparable oncological safety.
Is robotic nipple-sparing surgery safe?
Yes, in appropriately selected patients. Published meta-analyses show lower complication rates and comparable or better oncological outcomes versus conventional NSM. The primary trade-off is longer operative time. It requires an experienced surgical team and is not available at all centres.
Can breast cancer be treated without chemotherapy?
Some breast cancers — particularly small, hormone-positive, HER2-negative, node-negative tumours with favourable genomic profiles (e.g., low Oncotype DX score) — can be treated with surgery + hormone therapy alone, avoiding chemotherapy entirely. Your oncologist will guide this decision based on your specific tumour biology.
How long is recovery after robotic breast surgery?
Most patients are discharged within 24–48 hours. Light activities resume within a week. Drain management takes 1–2 weeks. Full recovery, including shoulder mobility rehabilitation and lymphedema prevention, takes 4–6 weeks.

Keep track of your appointments, get updates & more!

