





ENDOMETRIOSIS SURGERY WITH DA VINCI XI ROBOT - Expert Treatment for Deep Infiltrating Endometriosis
Dr. Swapna Misra | Director of Obstetrics, Robotic & Laparoscopic Gynaecology | Fortis Hospital Mohali
- India's Highest-Volume Robotic Gynaecology Centre
- Highest Number of Endometriosis Surgeries in the Region
- Zero Conversions to Open Surgery
Introduction: When Medication Isn't Enough
Endometriosis affects approximately 1 in 10 women of reproductive age worldwide — that's nearly 200 million women living with a condition that can dramatically impact their quality of life. If you're reading this, you or someone you love is likely among them. You've probably endured years of debilitating pelvic pain (chronic lower abdominal pain), painful periods (dysmenorrhea) that force you to miss work or school, pain during intimacy (dyspareunia) that strains relationships, and perhaps the heartbreak of infertility or difficulty getting pregnant. You've tried hormonal treatments, pain medications, and lifestyle modifications. But the pain persists.
The question you're now facing is: Is surgery the answer? And if so, which hospital in the Chandigarh, Mohali, or Punjab region should I go to, and who should perform it?
This comprehensive guide is authored by Dr. Swapna Misra, Director of Obstetrics, Robotic & Laparoscopic Gynaecology, Fortis Hospital Mohali — a surgeon who has performed the highest number of endometriosis surgeries in India with an unprecedented track record: not a single robotic case was converted to open surgery. Fortis Mohali performs the highest number of robotic gynaecologic procedures in the country, making it India’s premier centre for advanced minimally-invasive women’s health surgery.
In this guide, we’ll walk you through everything you need to know about endometriosis surgery using the Da Vinci Xi Robotic Surgical System — one of the most advanced technologies available for treating complex endometriosis. You'll learn what endometriosis really is, why surgery becomes necessary, how robotic keyhole surgery works, how it compares to traditional approaches, what to expect before and after the procedure, and why expertise matters more than technology alone.
Understanding Endometriosis: More Than Just Bad Periods
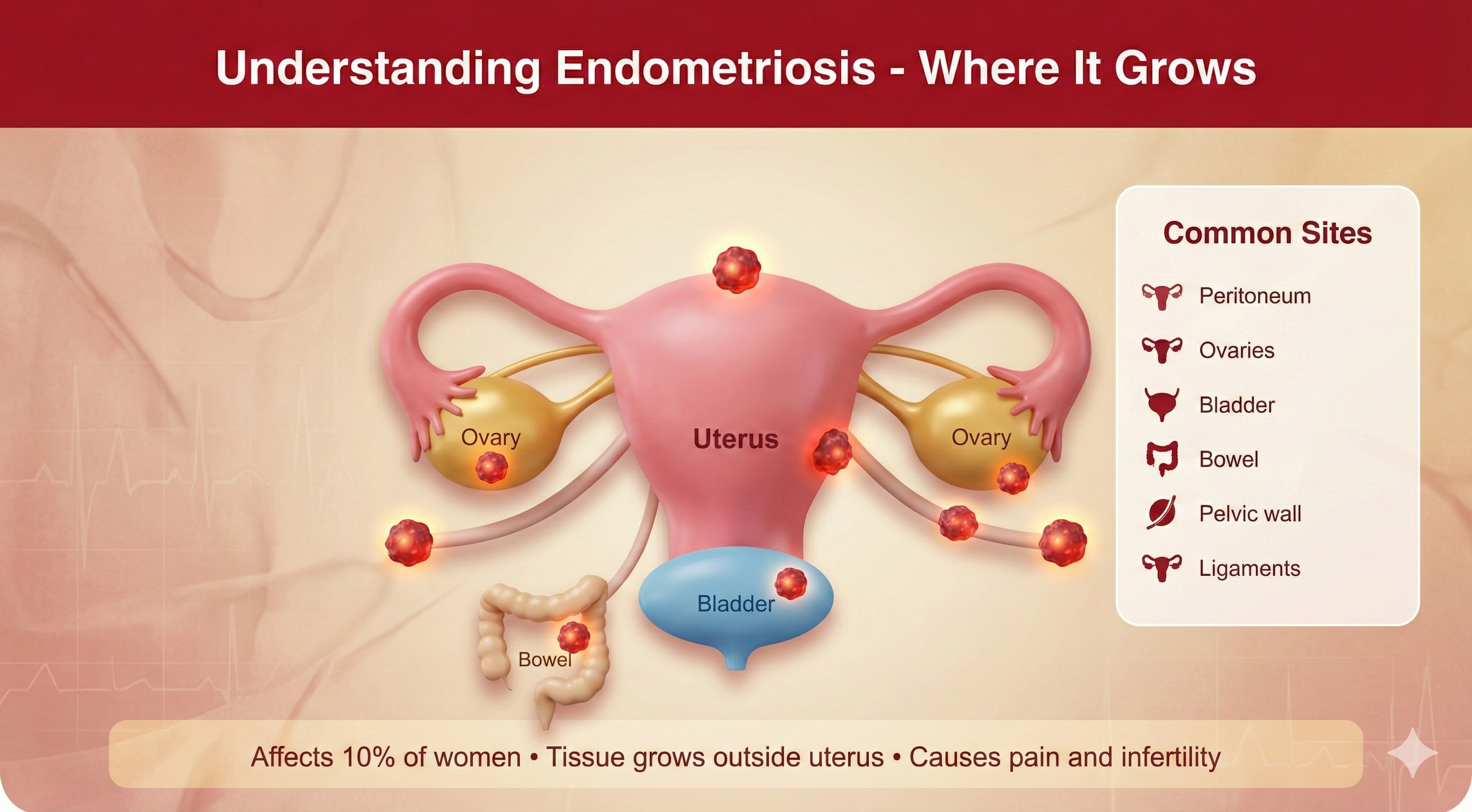
Endometriosis is a chronic condition in which the tissue similar to the lining of the uterus (called endometrium) grows outside the uterus — in places it doesn't belong. This rogue tissue can attach to the ovaries, fallopian tubes, outer surface of the uterus, pelvic lining (peritoneum), bladder, bowel, and even more distant organs. Just like the normal endometrial lining, this misplaced tissue responds to your menstrual cycle hormones — it thickens, breaks down, and bleeds each month. But unlike the tissue inside the uterus, which exits your body as your period, this blood has nowhere to go. It becomes trapped, causing inflammation, scarring, adhesions (bands of fibrous tissue that can glue organs together, often described by patients as "uterus sticking to bowel"), and sometimes deep, painful cysts called endometriomas.
Types and Locations of Endometriosis
- Superficial Peritoneal Lesions: These are small implants on the surface of the peritoneum (lining of the pelvic cavity). They appear as powder-burn lesions, red flame-like spots, or white scarred areas. While they may seem minor, they can cause significant pain.
- Ovarian Endometriomas (Chocolate Cysts): These are blood-filled cysts on the ovaries that can range from 2 cm to over 10 cm in size. They are called ‘chocolate cysts’ because the old blood inside looks like chocolate syrup. These cysts can damage healthy ovarian tissue and affect fertility, often requiring ovarian cyst removal surgery.
- Deep Infiltrating Endometriosis (DIE): This is the most challenging form, often seen in referral cases across Punjab and North India. When endometriosis invades more than 5 mm below the peritoneal surface, it is considered 'deep infiltrating.' DIE commonly affects:
- Bowel (rectum and sigmoid colon): Can cause painful bowel movements, constipation, diarrhoea, or rectal bleeding during periods.
- Bladder: Causes painful urination, urgency, and sometimes blood in the urine during menstruation.
- Ureters (tubes connecting kidneys to bladder): Can cause silent kidney damage if not detected.
- Rectovaginal septum (tissue between vagina and rectum): Causes severe pain during intercourse and bowel movements.
- Pelvic sidewalls and uterosacral ligaments: Can entrap nerves, causing chronic pain and sciatica.
Why Depth and Location Matter
Deep Infiltrating Endometriosis (DIE) is not just ‘worse’ superficial disease — it is a different beast entirely. The tissue burrows deep into organs, causing severe scarring and distortion of normal anatomy (often called a "frozen pelvis"). Ureters can be pulled out of position. The bowel can become tethered to the back of the uterus. Nerves become embedded in scar tissue. This is why DIE requires not just any gynaecologist, but a surgeon with extensive experience in complex pelvic dissection — someone like Dr. Swapna Misra, whose mastery of robotic techniques allows her to navigate these treacherous anatomical landscapes without converting to open surgery (large cut surgery).
Common Symptoms of Endometriosis
Patients visiting our Mohali clinic often report:
- Severe menstrual cramps (dysmenorrhea) that worsen over time and do not respond well to over-the-counter painkillers.
- Chronic pelvic pain that can persist even between periods.
- Pain during or after sexual intercourse (dyspareunia), often deep in the pelvis.
- Painful bowel movements or urination, especially during menstruation.
- Heavy menstrual bleeding or bleeding between periods.
- Infertility — endometriosis is found in 25 to 50 percent of women experiencing difficulty getting pregnant.
- Fatigue, bloating (often called "endo belly"), nausea, and digestive issues that worsen during your period.
- Sciatic nerve pain radiating down the leg (when nerves are involved).
Why Is Diagnosis Usually Delayed?
On an average, it takes 7 to 10 years from the onset of symptoms to receive an accurate diagnosis of endometriosis. This devastating delay happens because symptoms are often dismissed as ‘normal period pain’, women are told they have a ‘low pain tolerance’, or symptoms are misattributed to other conditions like Irritable Bowel Syndrome (IBS) or Pelvic Inflammatory Disease (PID). The only definitive way to diagnose endometriosis is through laparoscopic surgery (keyhole diagnosis) with tissue biopsy — meaning many women suffer for years before finally getting answers.
Goals of Endometriosis Surgery
When Dr. Swapna Misra performs endometriosis surgery at Fortis Mohali, the goals are clear and comprehensive:
- Complete excision of all visible endometriosis — not just ablation (burning), but complete removal of diseased tissue.
- Restoration of normal pelvic anatomy — separating organs that have been stuck together by adhesions.
- Preservation of fertility — protecting ovarian reserve while removing disease.
- Protection of vital organs — safeguarding the ureters, bladder, bowel, and nerves during dissection.
- Long-term symptom control — achieving durable pain relief and improved quality of life.
Excision vs. Ablation: Why Technique Matters
- Ablation: This technique uses heat (cautery or cauterization) or laser energy to burn away the surface of endometriosis lesions. It is quick and can be effective for very superficial disease. However, ablation only destroys the visible top layer — deeper disease beneath the surface remains, leading to higher recurrence rates.
- Excision: This involves surgically cutting out the endometriosis tissue completely, often going several millimetres deep to remove the entire lesion, including any roots beneath the surface. Excision is the gold standard for deep infiltrating endometriosis as it removes the disease entirely. Dr. Swapna Misra specializes in complete excision, which is why her patients experience lower recurrence rates and better long-term outcomes.
What Is Da Vinci Xi Robotic Surgery?
Let's be clear from the start – robotic surgery is not performed by a robot operating on its own. It is robot-assisted surgery — meaning a highly-trained surgeon is in complete control at all times, using an advanced robotic system as a tool to achieve unparalleled precision. Think of it as the surgeon’s hands being given superpowers: enhanced vision, greater dexterity, and steadier movements.
Dr. Swapna Misra operates from a console where she sees your pelvic anatomy in stunning 3D high-definition with 10x magnification. Her hand movements are translated in real time to robotic instruments inside your body — but with tremor filtration and motion scaling, implying her movements are smoother and more precise compared to the human hand using traditional instruments.
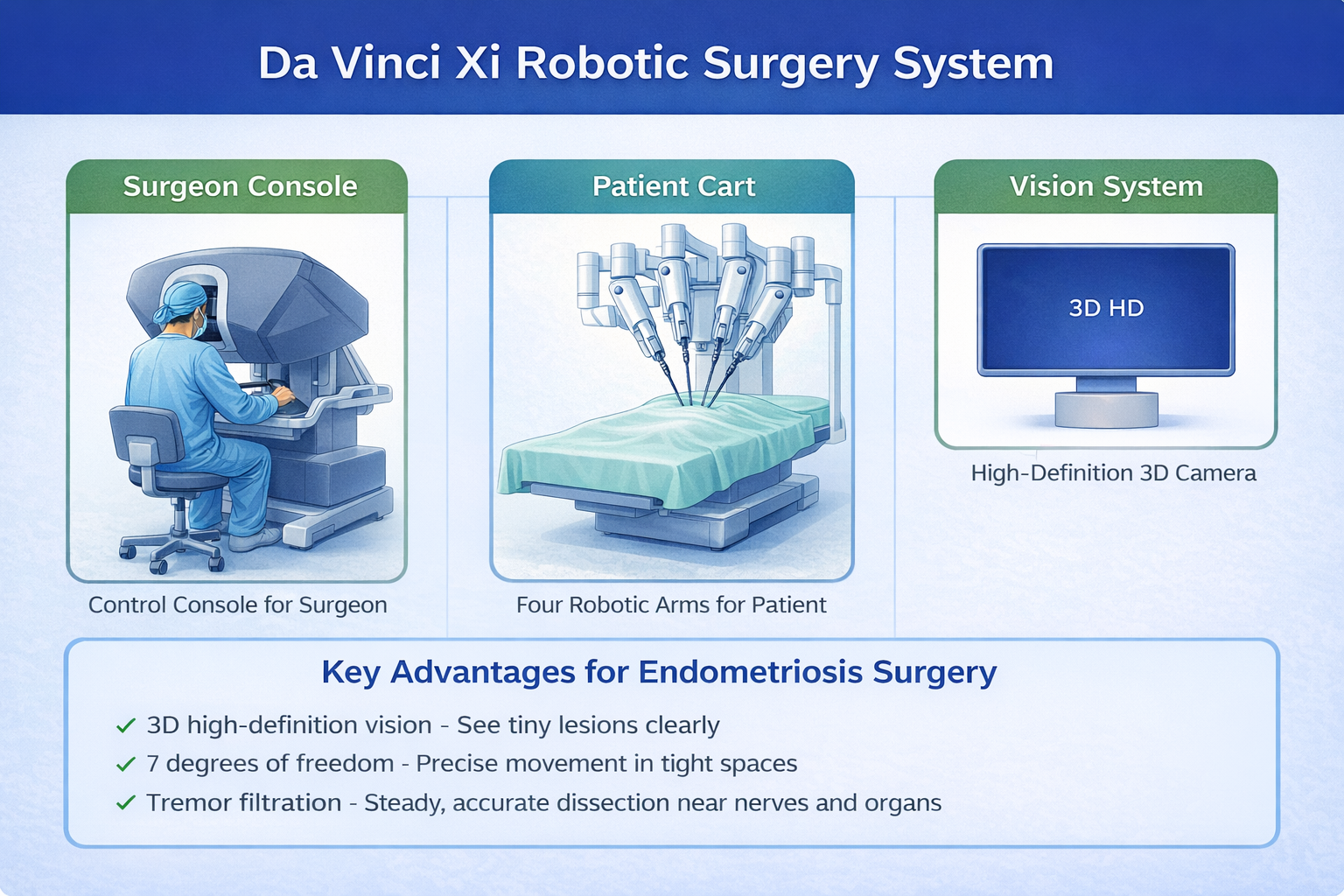
How the Da Vinci Xi System Works
- The Surgeon Console: Dr. Swapna Misra sits at a console in the operating room, looking through a high-definition 3D viewer that provides a magnified, immersive view of your pelvic anatomy. The console has hand and finger controls that she manipulates to move the robotic instruments and camera in real time. Every movement is instantly and precisely translated to the robotic arms inside your body — but with tremor filtration, meaning any natural hand tremors are automatically removed. This level of control is what allows Dr. Misra to perform the most complex dissections without ever needing to convert to an open surgery.
- The Patient Cart: This is the robotic system positioned next to you on the operating table. It has four robotic arms: one holds a high-definition 3D camera, and the other three hold specialized surgical instruments. These instruments have ‘wristed’ tips that can bend and rotate with 7 degrees of freedom — mimicking and even exceeding the range of motion of the human wrist. This allows Dr. Misra to access tight, hard-to-reach areas deep in the pelvis with far greater precision than traditional straight laparoscopic instruments.
- The Vision Cart: This component processes and displays high-definition 3D images captured by the camera, providing crystal-clear visualization of your anatomy. The level of detail is extraordinary — Dr. Misra can see individual nerve fibres, blood vessels, and layers of tissue that would be difficult to distinguish with the naked eye or standard 2D laparoscopic cameras. This superior visualization is key to her perfect track record — she can identify and protect critical structures that other surgeons might miss.
What Makes the Xi Platform Special for Endometriosis?
The Da Vinci Xi is the fourth-generation robotic platform from Intuitive Surgical, and it offers several key advancements over older models. The overhead boom design allows the system to be repositioned during surgery without undocking, enabling access to multiple areas of the pelvis and abdomen in a single procedure — critical for treating endometriosis, which can affect multiple sites simultaneously. The longer instrument reach and improved articulation make it ideal for deep pelvic work, such as excising endometriosis from the bowel, bladder, and pelvic sidewalls. At Fortis Mohali — India's highest-volume robotic gynaecology centre — Dr. Swapna Misra has access to the latest Xi platform and a dedicated team trained in complex endometriosis management.
Da Vinci Xi vs. Traditional Laparoscopic Surgery: An Honest Comparison
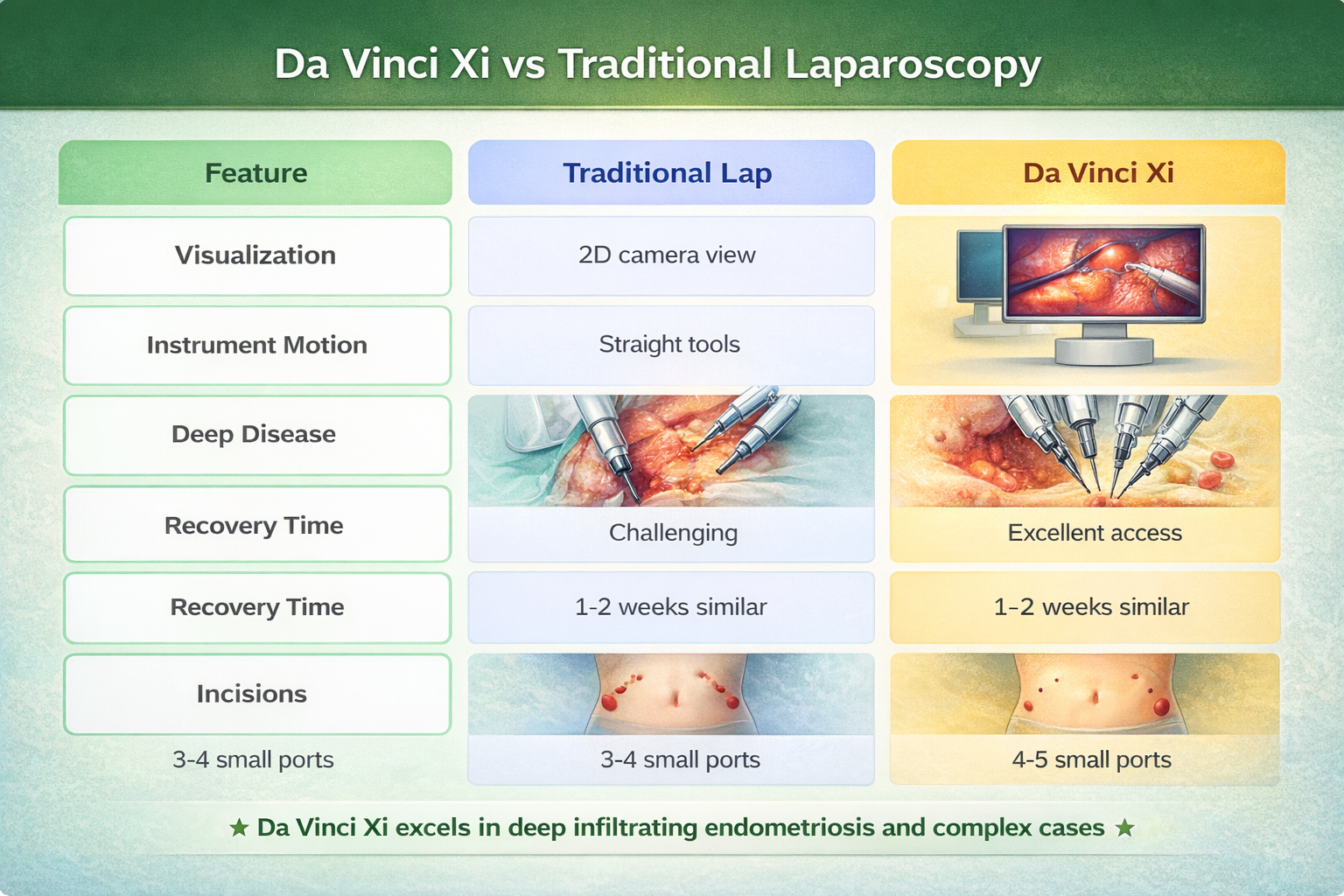
Both laparoscopic and robotic surgeries are minimally invasive (keyhole surgeries) — meaning they are performed through small incisions rather than one large abdominal opening. However, there are meaningful differences that can affect outcomes, especially in complex cases.
[Image comparing 2D laparoscopic view vs 3D robotic view]
- Visualization: 2D vs. 3D: Traditional laparoscopy uses a 2D camera, which projects a flat image onto a screen. While experienced surgeons are skilled at operating in 2D, depth perception is limited. The Da Vinci Xi provides true 3D high-definition vision with 10x magnification — Dr. Misra sees your anatomy as if looking directly into your body, with perfect depth perception. When dissecting endometriosis off the ureter or separating bowel from the uterus, this depth perception is not just helpful — it is critical for safety.
- Instrument Dexterity: Straight Tools vs. Wristed Instruments: Laparoscopic instruments are straight, rigid tools. Though they can push, pull, grasp, cut and cauterize, their range of motion inside the human body is limited. Da Vinci instruments have wristed tips with 7 degrees of freedom — they can bend, rotate, and articulate in ways that closely mimic the human wrist. This makes delicate manoeuvres like dissecting endometriosis off the bowel, suturing deep in the pelvis, or carefully separating adhesions far easier and more precise. This superior dexterity is why Dr. Swapna Misra has never felt the need to convert a robotic case to an open surgery. Even in the most challenging scenarios — extensive bowel involvement, frozen pelvis from severe adhesions, ureter completely encased in endometriosis — the Da Vinci Xi’s instruments allow her to operate safely in spaces where traditional laparoscopic tools would struggle.
- Surgeon Ergonomics and Fatigue: In traditional laparoscopy, the surgeon stands at the operating table holding instruments for hours, which can lead to physical fatigue — especially in long, complex cases. The Da Vinci console allows the surgeon to sit comfortably with arms supported, reducing fatigue and potentially improving focus and precision during lengthy procedures. Some of Dr. Misra’s most complex endometriosis excisions take up to 4 to 5 hours — the ergonomic advantage of the robotic console ensures she maintains peak performance throughout.
Conversion to Open Surgery: The Ultimate Measure of Success
One of the most important metrics in minimally invasive surgery is the conversion rate — how often a surgeon must abandon the minimally invasive approach and convert to open surgery due to complications, difficulty or bleeding. Traditional laparoscopy for severe endometriosis has a conversion rate of 5 to 10 percent in published literature. Dr. Swapna Misra’s conversion rate with Da Vinci Xi? Zero. Not a single case converted to open surgery. This unprecedented track record speaks volumes about her surgical expertise and the advantages of the robotic platform in the most challenging cases.
Operative Time, Blood Loss, and Complications
Multiple studies have compared outcomes between laparoscopic and robotic endometriosis surgery. The data show that in experienced hands, complication rates and blood loss are generally comparable. Operative time can sometimes be slightly longer with robotic surgery due to the set-up and docking, but at high-volume centres like Fortis Mohali where the team is highly experienced, this difference is minimal.
What sets Fortis Mohali apart is not just the technology — it is the volume. Performing the highest number of robotic gynaecologic procedures in India means the entire team — surgeons, anaesthesiologists, nurses, technicians — has seen and successfully managed every conceivable scenario. This experience translates directly to better outcomes for patients from Chandigarh, Panchkula, and across Punjab.
Recovery and Cosmesis
Both approaches involve small incisions (typically 4 to 5 ports, each 8 to 12 mm), so recovery times and scarring are similar. You can expect to return to light activities within a week and resume normal activities within 2 to 4 weeks with either method. The main advantage of robotic surgery is not faster recovery, but rather the potential for more thorough and precise excision of complex disease — which translates to better long-term symptom relief and lower recurrence rates.
Who Is the Ideal Candidate for Da Vinci Xi Surgery?
Not everyone with endometriosis needs robotic surgery. For superficial peritoneal lesions or mild disease, traditional laparoscopy is perfectly adequate and may be more cost-effective. However, robotic surgery with Dr. Swapna Misra at Fortis Mohali shines in the following scenarios:
- Deep Infiltrating Endometriosis (DIE): When endometriosis invades more than 5 mm below the surface of the peritoneum, it is considered ‘deep infiltrating.’ This often affects the bowel, bladder, ureters, rectovaginal septum, and pelvic sidewalls. DIE is notoriously difficult to treat because the tissue is deeply embedded, often causing severe scarring and distortion of anatomy. The enhanced visualization and dexterity of the Da Vinci Xi make it far easier to meticulously excise these deep lesions while preserving surrounding structures.
- Complex Adhesions and Prior Surgeries: If you’ve had previous pelvic surgeries (like previous C-sections or cyst removals), you likely have adhesions — scar tissue that can bind organs together. Operating in this environment requires patience, precision and excellent visualization to safely separate structures without causing injury. Dr. Misra’s expertise with the robotic platform allows her to navigate even the most challenging ‘frozen pelvis’ scenarios.
- Multi-organ Involvement: When endometriosis affects multiple organs — for example, ovarian endometriomas plus bowel nodules plus bladder involvement — a multi-disciplinary surgical team may be needed. At Fortis Mohali, Dr. Misra works closely with colorectal surgeons, urologists, and other specialists as needed. The Da Vinci Xi's ability to access multiple areas without repositioning makes it ideal for these complex, multi-stage procedures.
- Need for Bowel Resection or Urinary Tract Surgery: When endometriosis deeply infiltrates the bowel or ureters, simple excision may not be sufficient — a segment of bowel may need to be removed and reconnected (segmental resection), or the ureter may need to be freed and reconstructed. These advanced procedures require meticulous suturing in deep, confined spaces — exactly where the Da Vinci Xi excels. Dr. Misra has extensive experience with bowel shaving, discoid resection and segmental bowel resection, all performed robotically without conversion to an open surgery.
Your Surgical Journey with Dr. Swapna Misra at Fortis Mohali
Pre-Operative Evaluation
Before surgery, Dr. Misra will conduct a thorough medical examination at her clinic. This includes:
- Detailed symptom mapping — exactly where and when you experience pain, impact on bowel and bladder function, sexual health, fertility goals.
- Imaging studies — transvaginal ultrasound (TVS) with endometriosis protocol to identify ovarian endometriomas and assess ovarian reserve; MRI Pelvis for deep disease involving the bowel, bladder, or ureters.
- Fertility counselling — if you are trying to conceive, discussion of egg preservation, ovarian reserve, and timing of surgery versus IVF.
- Bowel and urinary assessment — colonoscopy or cystoscopy may be recommended if deep bowel or bladder involvement is suspected.
- Multi-disciplinary planning — coordination with colorectal surgery or urology if needed.
Day of Surgery at Fortis Mohali
On the day of your surgery, you will arrive at Fortis Hospital Mohali after fasting overnight. Under general anaesthesia, you will be positioned on the operating table. Dr. Misra and her team will make 4 to 5 small incisions in the abdomen (each about 8 to 12 mm). Carbon dioxide gas will be used to gently inflate your abdomen, creating space for the camera and instruments to manoeuvre. The Da Vinci Xi will be docked and Dr. Misra will take her position at the console.
Procedures That May Be Performed
- Complete excision of endometriosis implants from the peritoneum, ovaries, uterus, and other pelvic surfaces.
- Adhesiolysis — carefully cutting away scar tissue to restore normal anatomy and free up organs.
- Endometrioma cystectomy — removal of ovarian cysts (chocolate cysts) while meticulously preserving healthy ovarian tissue to protect fertility.
- Ureterolysis — freeing the ureters from surrounding endometriosis, with placement of ureteral stents if needed for safety.
- Bladder nodule excision — removing deeply embedded endometriosis from the bladder wall, with repair if full-thickness resection is needed.
- Bowel endometriosis management — ranging from shaving (removing surface disease), to discoid resection (removing a button of bowel wall), to segmental resection (removing a section of bowel and reconnecting it).
- Rectovaginal septum excision — removing disease from the tissue between the vagina and rectum.
Depending on the extent of the disease, the surgery can last between 2 to 5 hours or more. At Fortis Mohali, Dr. Misra’s goal is always complete excision — removing all visible endometriosis, not just burning or ablating the surface. This thoroughness is what leads to better long-term outcomes.
Hospital Stay and Recovery
Majority of the patients stay a night in the hospital for better observation and pain management. You will be encouraged to walk within hours of the surgery to prevent blood clots and promote healing. Pain is managed with a combination of medications, and most women describe the discomfort as similar to moderate menstrual cramps — manageable with medication. You can resume a normal diet as tolerated, though your doctor may recommend a bowel regimen to prevent constipation, especially if bowel work was done.
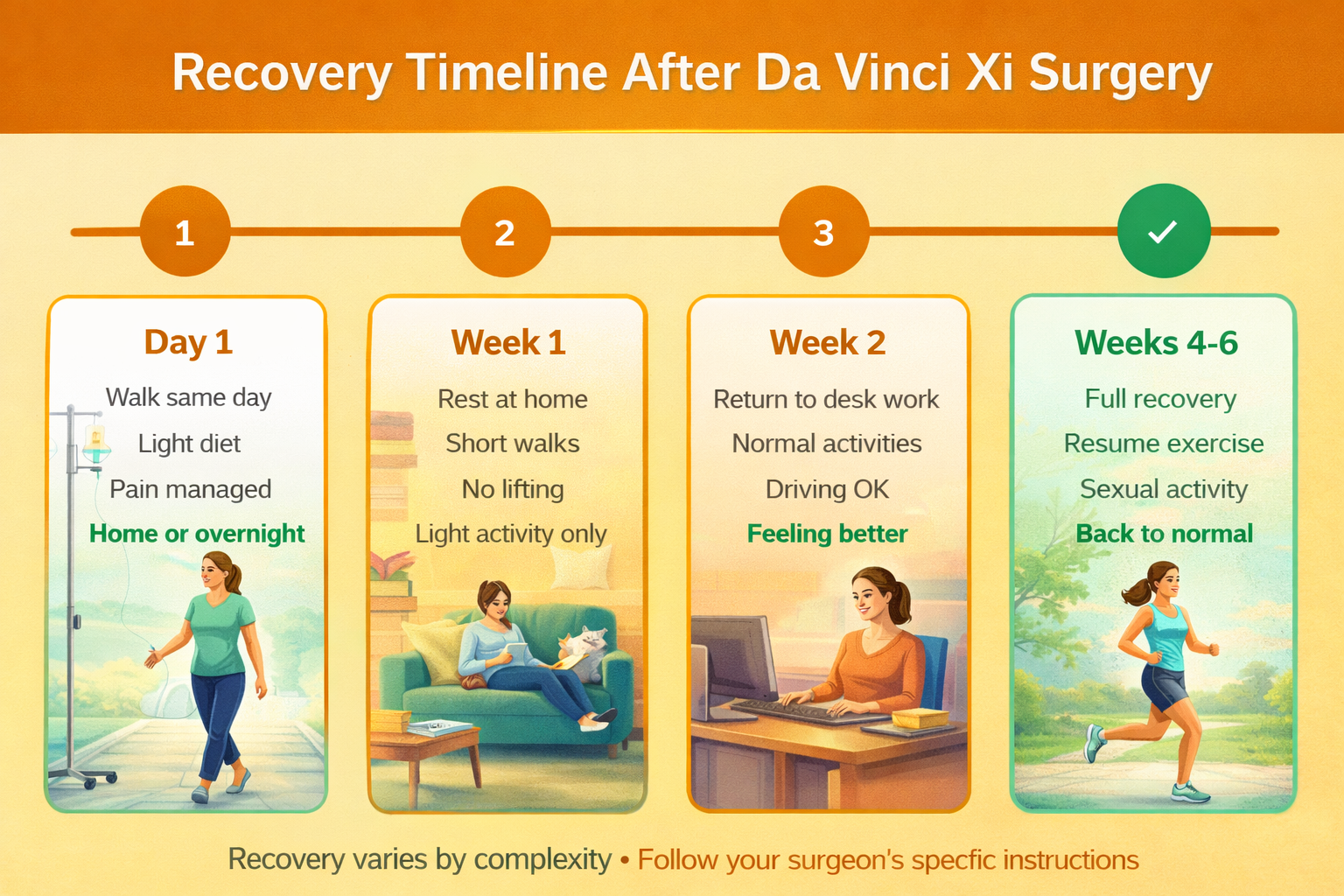
Recovery Timeline
- Day 1: Walk same day, light diet, pain managed, home or one-night hospital stay.
- Week 1: Rest at home, short walks encouraged, avoid lifting anything over 5 kg (10 pounds), abstain from driving while on pain medication.
- Week 2: Gradual return to normal activities, many women return to desk jobs by week 2, driving permitted once off narcotics.
- Weeks 3-4: Light exercise (walking, gentle yoga), resumption of daily activities.
- Weeks 4-6: Resume gym, running, sexual activity, and lifting with your doctor’s clearance.
- 6+ weeks: Full recovery, resumption of all normal activities, including high-impact exercise.
Outcomes and Expectations: What Success Looks Like
- Pain Relief: Studies show that surgical excision of endometriosis provides significant pain relief in 70 to 80 percent of women. At Fortis Mohali, Dr. Swapna Misra’s patients report even higher rates of satisfaction, likely due to her focus on complete excision rather than ablation. However, surgery is not a guaranteed cure. Endometriosis can reoccur, and some women experience persistent pain due to central sensitization — a phenomenon where the nervous system remains hypersensitive even after the disease is removed. Long-term pain management may include hormonal suppression after surgery (for those not trying to conceive), pelvic floor physical therapy, and lifestyle modifications. Dr. Misra provides comprehensive follow-up to ensure optimal long-term outcomes.
- Fertility Outcomes: If you are trying to conceive, surgery can improve fertility by restoring normal pelvic anatomy, removing disease that may be blocking the fallopian tubes, and improving the pelvic environment for conception. However, surgery is not always the best first step. In some cases, especially with large ovarian endometriomas, surgery may reduce ovarian reserve (remaining number of eggs). Dr. Misra works closely with fertility specialists to help you weigh the benefits and risks of surgery versus proceeding directly to IVF. For women who do undergo surgery, Dr. Misra’s meticulous technique preserves as much healthy ovarian tissue as possible, maximizing the chances of future fertility.
- Recurrence and Long-Term Management: Endometriosis can and does reoccur in some women. The reoccurrence rate varies depending on the completeness of excision and whether hormonal suppression is used after surgery. Women who do not use hormonal therapy after surgery have a higher reoccurrence rate — approximately 20 to 30 percent over 5 years. With hormonal suppression (such as birth control pills, progestin therapy, or GnRH agonists), reoccurrence rates drop significantly. This is why Dr. Misra emphasizes that surgery is a vital part of a comprehensive treatment plan. For women not actively trying to conceive, continued hormonal therapy after surgery can help prevent endometriosis from returning.
Risks and Limitations: What You Need to Know
All surgeries carry risks, and it is important to understand them before arriving at a decision. Dr. Misra believes in complete transparency with her patients.
- General Surgical Risks: Bleeding (risk is minimized with robotic precision), infection (rare with minimally invasive surgery, typically less than 1 percent), blood clots (prevented through early mobilization), and anaesthesia-related complications (managed by our experienced anaesthesia team).
- Endometriosis-Specific Risks: Injury to surrounding organs such as the bowel, bladder, or ureters — the risk increases with severe, deep disease. Dr. Misra’s extensive experience and robotic precision minimize this risk. There is also a possibility of needing bowel resection or urinary tract repair if disease is more extensive than anticipated — Dr. Misra is fully trained in these procedures and performs robot-aided surgery. Other risks include incomplete excision if disease is more widespread than imaging suggested (rare at Fortis Mohali due to thorough pre-operative evaluation), persistent pain despite surgery due to nerve sensitization, and adhesion reoccurrence.
- Robotic Surgery Considerations: The high cost of robotic surgery compared to laparoscopy is a consideration, though many insurance plans cover it for complex cases. The lack of tactile feedback (surgeon cannot ‘feel’ tissues directly) is sometimes cited as a limitation, though visual feedback at 10x magnification largely compensates. Most importantly, outcomes depend heavily on surgeon expertise. Robotic surgery is not automatically better — it is a tool that must be wielded only by a skilled and experienced surgeon. This is why choosing a high-volume centre like Fortis Mohali with a surgeon like Dr. Swapna Misra helps makes all the difference.
Why Choose Fortis Mohali and Dr. Swapna Misra?
- India's Leading Robotic Gynaecology Centre: Fortis Hospital Mohali performs the highest number of robotic gynaecologic procedures in India. This volume matters. Every member of the surgical team — ranging from the anaesthesiologists who manage complex cases, to the nurses who assist in positioning, to the technicians who maintain the equipment — has seen and successfully managed thousands of procedures. Experience translates directly to safety and better outcomes.
- Dr. Swapna Misra: Unparalleled Expertise: Dr. Misra has performed the highest number of endometriosis surgeries in India. Her track record speaks for itself:
- Zero robotic cases converted to open surgery — an unprecedented achievement demonstrating mastery over the most complex cases.
- Extensive experience with deep infiltrating endometriosis involving bowel, bladder and ureters.
- Expertise in fertility-preserving surgery — meticulous ovarian-sparing techniques.
- Multi-disciplinary approach — collaboration with colorectal surgery, urology and fertility specialists as needed.
- Commitment to complete excision rather than ablation — the gold standard for long-term outcomes.
- State-of-the-Art Technology: Fortis Mohali is equipped with the latest Da Vinci Xi platform, advanced imaging capabilities, and a dedicated robotic surgery suite designed specifically for complex gynaecologic procedures.
- Comprehensive Care Pathway: From the first consultation through surgery and long-term follow-up, patients receive comprehensive, patient-centered care. Dr. Misra and her team understand that endometriosis is not just a surgical problem — it is a chronic condition that requires ongoing management.
Frequently Asked Questions About Endometriosis Surgery
- Is Da Vinci Xi surgery safe for endometriosis? Yes, it is very safe when performed by experienced surgeons. At Fortis Mohali, complication rates are extremely low, and Dr. Swapna Misra has never converted a robotic case to open surgery due to her expertise and precision of the robotic platform.
- Is robotic surgery better than laparoscopy for endometriosis? For deep infiltrating endometriosis and complex cases involving multiple organs, robotic surgery offers significant advantages in visualization, precision and dexterity. For mild, superficial disease, traditional laparoscopy may be equally effective. The key is choosing a surgeon with extensive endometriosis experience — the surgeon’s skill matters more than the technology.
- What is the difference between excision and ablation? Excision means cutting out the endometriosis tissue completely, often going deep to remove the entire lesion, including roots beneath the surface. Ablation means burning away the surface using heat or laser. Excision is generally preferred for deep disease as it removes the tissue entirely, reducing reoccurrence risk. Dr. Misra specializes in such complete excision.
- How long does recovery take after robotic endometriosis surgery? Most women recover within 2 to 4 weeks. You can expect to return to desk work within 1 to 2 weeks and resume exercise and sexual activity by 4 to 6 weeks. Full internal healing takes about 6 weeks.
- Will robotic surgery cure endometriosis permanently? Surgery is not a cure. Endometriosis can reoccur in 20 to 30 percent of women over 5 years if no hormonal suppression is used after surgery. However, surgery provides significant long-term symptom relief in most women. Using hormonal therapy after surgery (for those not trying to conceive) reduces reoccurrence risk substantially.
- Can robotic surgery improve fertility? Yes, by restoring normal anatomy, removing adhesions, and clearing disease that interferes with conception. However, for some women — particularly those with large ovarian endometriomas — IVF may be a better first option because surgery can reduce ovarian reserve. Dr. Misra works closely with fertility specialists to determine the best path for each patient.
- What if bowel or bladder endometriosis is found during surgery? Dr. Misra is fully trained in managing bowel and bladder endometriosis robotically. She performs bowel shaving, discoid resection, and segmental bowel resection as needed, often in collaboration with a colorectal surgeon. Similarly, bladder nodules can be excised and the bladder repaired robotically. These complex procedures are performed without converting to an open surgery.
- Does robotic surgery cost more than laparoscopy? Yes, robotic surgery is typically more expensive than traditional laparoscopy due to the cost of the equipment and specialized training. However, many insurance plans cover robotic surgery for complex cases such as deep infiltrating endometriosis. The team at Fortis Mohali can help you navigate insurance approval.
- How do I know if I need robotic surgery versus traditional laparoscopy? During your consultation with Dr. Misra, she will review symptoms, imaging studies and previous treatments to determine the extent and location of your endometriosis. If you have deep infiltrating disease, bowel or bladder involvement, severe adhesions, or prior failed surgeries, robotic surgery is likely the best option. For mild, superficial disease, traditional laparoscopy may be sufficient.
- What should I ask when choosing an endometriosis surgeon?
- How many endometriosis surgeries do you perform per year?
- What percentage of your cases are deep infiltrating endometriosis?
- Do you perform excision or ablation?
- What is your conversion rate to open surgery?
- Do you work with a multi-disciplinary team for bowel and urinary involvement?
- What is your approach to fertility preservation?
- What is your plan for long-term management and preventing recurrence?
Conclusion: Expert Care for Complex Endometriosis
Endometriosis is a complex, chronic disease that can profoundly impact your life. But with the right surgeon and right technology, there is real hope for lasting relief. Dr. Swapna Misra’s unparalleled expertise in robotic endometriosis surgery, combined with Fortis Mohali’s status as India's highest-volume robotic gynaecology centre, offers patients access to world-class care right here in Punjab.
Her track record — the highest number of endometriosis surgeries in India with zero conversions to open surgery — demonstrates not just technical skill, but a level of mastery that comes from dedicating a career to this challenging subspecialty.
The most important decision you will make is not whether to choose robotic or laparoscopic surgery. It is choosing a surgeon who specializes in endometriosis excision, who has the skill and experience to treat the most complex cases, and who will partner with you in creating a comprehensive, long-term treatment plan.
If you are suffering from endometriosis and medical treatments have not provided relief, you deserve expert care. Consult Dr. Swapna Misra at Fortis Mohali to discuss whether Da Vinci Xi robotic surgery is right for you. Don’t let endometriosis control your life any longer.
Schedule Your Consultation with Dr. Swapna Misra
Contact Us – Fortis Hospital Mohali
For appointments, consultations, and diagnostic services, please contact:
📞 72728 72728
Our care team will assist you with:
Doctor appointments
Diagnostic and screening services
Health check-ups
Call now to book your appointment at Fortis Hospital, Mohali.
Categories
Clear allMeet the doctor

- Oncology | Surgical Oncology
- Obstetrics and Gynaecology | Gynaecologic Oncology | Obstetrics and Gynaecology
-
 23 Years
23 Years
-
 1250
1250
Related Blogs
View all

Bacterial Vaginosis: Causes, Symptoms And Treatment


Awareness, Breast Self-Examination And Regular Screening Examination Can Change The Life o...

Hormonal Imbalance: Symptoms, Causes And Treatment

Evolution of Gynae & Cancer Surgeries With Robotics


Know The Top 11 Benefits of Antenatal Exercises


Quick Enquiry Form

Keep track of your appointments, get updates & more!

