






“Something Is Coming Down” Understanding Pelvic Organ Prolapse — And How to Fix It
By Dr Daisy Shethna Consultant Urogynaecologist | Fortis Hospital, Mohali MS (OBGY) | MRCOG (London) | Fellowship in Urogynaecology (Singapore)
The Condition No One Talks About — But 1 in 3 Mothers Experience
“I feel like something is falling out of me.” “There’s a ball down there by evening.” “My doctor said it’s normal for my age.” If any of this sounds familiar, you are not alone. Pelvic organ prolapse affects up to 1 in 3 women who have had a baby — yet it remains one of the least discussed conditions in women’s health.
Every week, women walk into my clinic embarrassed and say: “Doctor, I feel like something is coming down.” Many have suffered in silence for years — adapting their entire lives around a condition they thought was untreatable. It is treatable. And you do not have to live with it.
What Is Pelvic Organ Prolapse?
The pelvic floor is a group of muscles, ligaments, and connective tissues forming a supportive hammock at the base of the pelvis. This hammock holds the bladder, uterus, vagina, and rectum in their correct positions. Childbirth, ageing, hormonal changes, or chronic pressure can weaken this support. When that happens, one or more pelvic organs slips downward into the vaginal canal. That is pelvic organ prolapse (POP).
- POP is the second most common urogynaecological condition after urinary incontinence
- It affects up to 1 in 3 women who have given birth
- It is not life-threatening — but it significantly affects comfort, confidence, and quality of life
- It is not an inevitable part of ageing — and most cases are treatable
Why Does It Happen?
Pregnancy and vaginal delivery: The single greatest risk factor. Instrumental delivery (forceps or vacuum), prolonged labour, large babies, severe perineal tears, and multiple vaginal births all increase risk substantially.
Ageing and menopause: Falling oestrogen levels after menopause cause tissues to lose strength, elasticity, and collagen — accelerating prolapse. Topical vaginal oestrogen can help restore tissue quality.
Chronic pelvic floor pressure: Constipation, chronic cough, obesity, heavy occupational lifting, and repeated straining gradually erode support structures over years.
Genetics: Some women inherit weaker connective tissue. A family history of prolapse significantly increases personal risk.
Prior hysterectomy: Women who have had a hysterectomy can develop vault prolapse (the top of the vagina descends) if adequate apical support was not established during the original surgery.
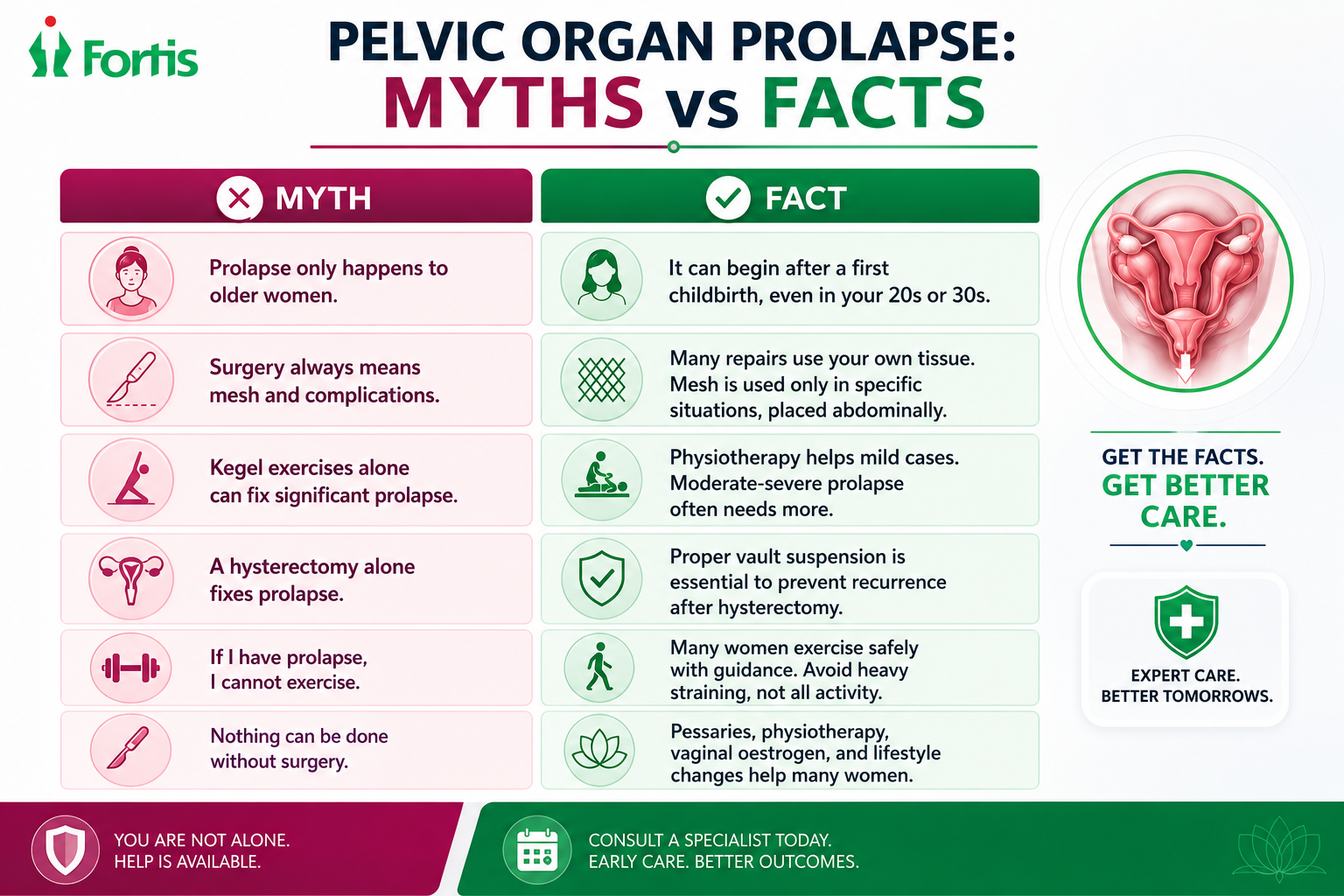
Myths vs Facts
Many women delay treatment because of beliefs that are simply not true.
Types of Prolapse: How to Tell Them Apart
Cystocele (bladder prolapse): The bladder bulges into the front wall of the vagina. Symptoms include vaginal heaviness, difficulty emptying the bladder, frequent urination, recurrent UTIs, and stress urinary leakage.
Rectocele (posterior vaginal wall prolapse): The rectum bulges into the back wall of the vagina. Note: this is NOT the same as rectal prolapse (where the rectum itself protrudes through the anus). Symptoms include pressure, straining to pass stool, incomplete bowel emptying, and needing to push vaginally to defecate.
Uterine prolapse: The uterus descends into the vaginal canal. Symptoms include pelvic heaviness, a visible bulge, discomfort while walking, pain during intercourse, and worsening by evening.
Vault prolapse: In women who have had a hysterectomy, the top of the vagina can descend. This requires specific surgical repair, usually sacrocolpopexy.
The most common patient description — regardless of prolapse type — is: “By the end of the day, something feels like it is falling out. It’s better in the morning after lying down.” This worsening with gravity and standing is characteristic of prolapse.
When Should You See a Urogynaecologist?
- A vaginal bulge or sensation of “something coming down”
- Heaviness that worsens by evening or after prolonged standing
- Difficulty emptying the bladder or bowel
- Recurrent urinary infections
- Need to push the bulge back to pass urine or stool
- Pain, bleeding, or ulceration from the prolapsed tissue
- Prolapse affecting walking, exercise, travel, or intimacy
See a specialist URGENTLY if you have: inability to pass urine, severe pain, bleeding or ulceration on the prolapsed tissue, foul-smelling discharge, fever with urinary symptoms, or sudden worsening.
How Is Prolapse Diagnosed?
At your first consultation, the urogynaecologist will take a detailed history and perform a pelvic examination using a standardised grading system called POP-Q, which measures exactly how far each compartment has descended. A cough stress test checks for urinary leakage that may be present alongside prolapse. A post-void residual urine test assesses whether the bladder is emptying properly. A urine test rules out infection. Ultrasound or urodynamics are added only in selected cases with complex bladder or bowel symptoms.
Why prolapse and urinary incontinence often go together: Prolapse changes the angle of the urethra and bladder neck. This can cause leakage, incomplete emptying, urgency, or recurrent infections. Sometimes, prolapse actually masks stress incontinence — and after repair, hidden leakage may become noticeable. Your urogynaecologist assesses both before surgery to plan accordingly.
Treatment: Not Every Prolapse Needs Surgery
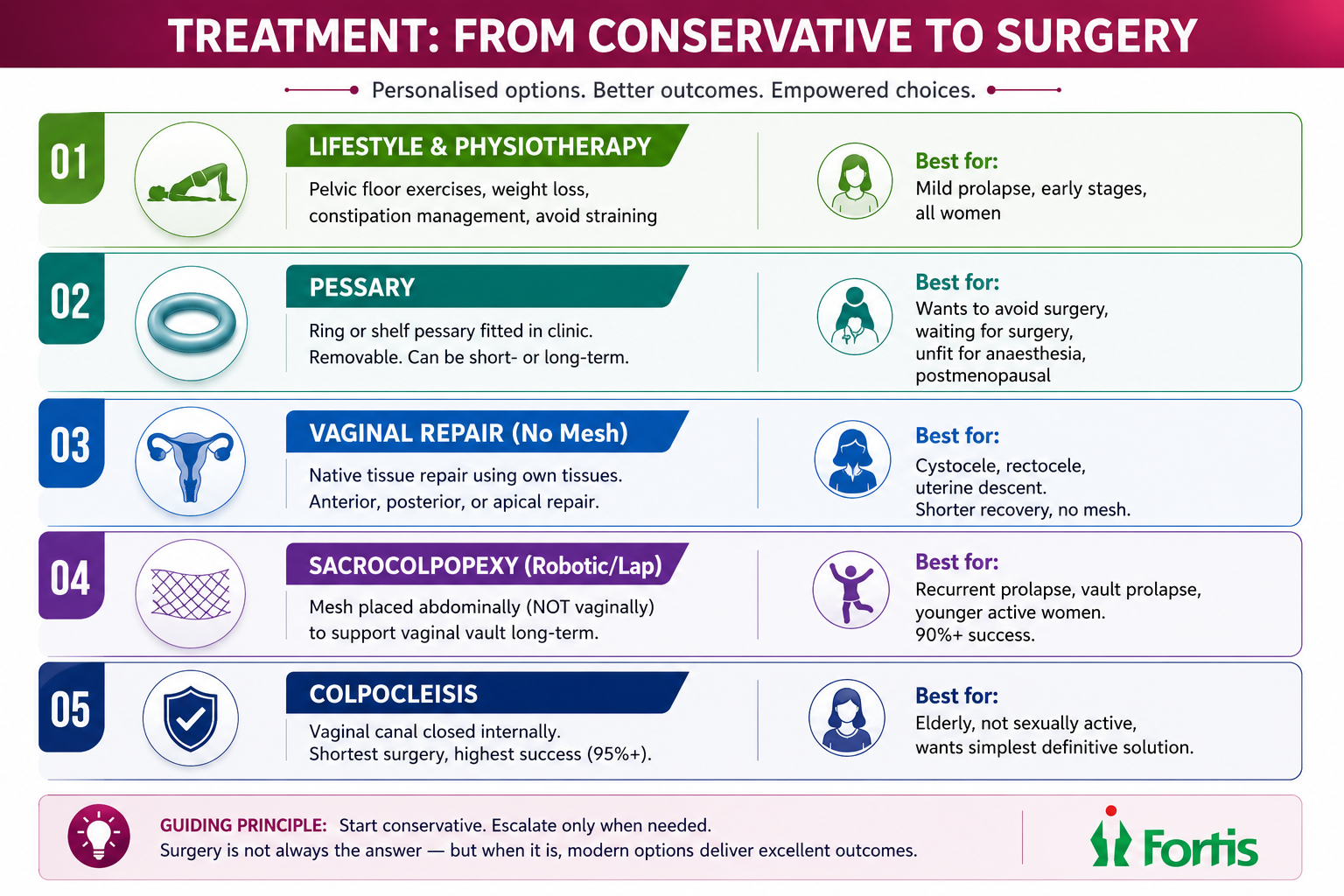
Step 1: Lifestyle and Pelvic Floor Physiotherapy
Supervised pelvic floor muscle training (PFMT) is the first-line treatment for mild prolapse. A structured programme strengthens the pelvic floor muscles, improves support, and can reduce symptoms significantly. Weight management, constipation control, avoiding heavy lifting, and treating chronic cough all reduce the forces that worsen prolapse.
Step 2: Pessary — A Non-Surgical Support
A vaginal pessary is a silicone device inserted in the clinic that physically supports the prolapsed organs from inside. Approximately 80% of women can be successfully fitted with a pessary. It is removable, can be used short-term (while waiting for surgery) or long-term (indefinitely in women who prefer to avoid surgery), and is particularly valuable for women who are unfit for anaesthesia, postmenopausal (combined with vaginal oestrogen for comfort), or simply not ready for surgery. Follow-up is needed for cleaning and checking.
Step 3: Surgery — When Conservative Measures Are Not Enough
Surgery is considered when symptoms significantly affect quality of life despite conservative measures, when there is a visible bulge outside the vaginal opening, when bladder or bowel emptying is impaired, or when the patient wants a definitive long-term solution.
Native tissue repair (vaginal): The most commonly performed prolapse surgery worldwide. Weakened vaginal walls are repaired using the patient’s own tissues. No mesh. No abdominal incisions. Anterior repair corrects cystocele; posterior repair corrects rectocele. Faster recovery.
Uterine-preserving surgery: Many women ask: ‘Can my uterus be saved?’ For selected patients — yes. Manchester’s repair / Sacrospinous hysteropexy (vaginal) or sacrohysteropexy (laparoscopic/robotic) lifts and re-suspends the uterus. Commonly offered to younger women or those with strong personal preference.
Vaginal hysterectomy + apical suspension: Where significant uterine descent is present, the uterus is removed vaginally and the vaginal vault is simultaneously suspended to strong pelvic ligaments. No mesh. Good long-term support. Critical: proper vault suspension must accompany hysterectomy to prevent future vault prolapse.
Sacrocolpopexy (laparoscopic / robotic via da Vinci Xi): The gold standard for vault prolapse and recurrent prolapse. The vaginal vault is attached to the sacral promontory using surgical mesh placed abdominally — not vaginally. This is different from older transvaginal mesh procedures that raised safety concerns. Abdominal sacrocolpopexy has excellent long-term durability, with success rates exceeding 90% at 5 years. At Fortis Mohali, this is performed robotically through the da Vinci Xi for precision and minimally invasive recovery.
Colpocleisis (obliterative surgery): For elderly women who are not sexually active and want the simplest, most definitive solution. The vaginal space is closed internally under short anaesthesia. Success rates exceed 95%. This is irreversible — vaginal intercourse will no longer be possible. Clear and complete consent is essential.
From the Practice
A 62-year-old retired school principal from Panchkula came to see me after two years of worsening heaviness and a visible vaginal bulge. She had stopped walking, stopped visiting friends, and stopped attending her grandchildren’s school events. She had been told by her GP that “this is normal at your age.” On examination, she had Stage III uterovaginal prolapse with a moderate cystocele. We first tried a ring pessary — fitted in the clinic in five minutes. She came back two weeks later and said: “Doctor, I cried. Not from pain — from relief. I walked to the market for the first time in a year.” She continues to manage successfully with the pessary and topical oestrogen. Surgery was not needed.
Why Women in India Delay Treatment
Embarrassment. Belief that prolapse is “normal after children.” Lack of awareness that a specialist called a urogynaecologist even exists. Fear of surgery. Dependence on home remedies. Not discussing sexual or bowel symptoms with anyone — not even a doctor. These cultural barriers cost women years of unnecessary suffering. A urogynaecologist is trained specifically for this. You will not surprise or embarrass us. And the first conversation is all it takes to start the path toward feeling normal again.
If you feel a vaginal bulge, heaviness, or difficulty emptying your bladder or bowel, do not assume it is “normal for your age.” Consult Dr Daisy Shethna at the Urogynaecology and Pelvic Floor Centre, Fortis Hospital Mohali, for a confidential assessment and a personalised treatment plan. You deserve to feel confident, comfortable, and in control of your body again.
About the Author
Dr Daisy Shethna is a Consultant Urogynaecologist at Fortis Hospital, Mohali. She completed her MS (OBGY) and holds Membership of the Royal College of Obstetricians and Gynaecologists, London (MRCOG). Dr Shethna completed a Fellowship in Urogynaecology in Singapore, with training in advanced pelvic floor surgery, urodynamics, and minimally invasive prolapse and incontinence procedures. She has established the Urogynaecology and Pelvic Floor Centre at Fortis Mohali — the first dedicated urogynaecology service in the Tricity region. Her clinical focus includes pelvic organ prolapse, urinary incontinence, voiding dysfunction, pessary management, and pelvic floor rehabilitation. References: NICE NG123, ACOG, IUGA, RCOG.
Categories
Clear allMeet the doctor
}}drupal-data/images/doctor_female.jpg)
- Obstetrics and Gynaecology | Obstetrics and Gynaecology
-
 5 Years
5 Years
-
 950
950
Related Blogs
View all

Bacterial Vaginosis: Causes, Symptoms And Treatment


Awareness, Breast Self-Examination And Regular Screening Examination Can Change The Life o...

Hormonal Imbalance: Symptoms, Causes And Treatment

Evolution of Gynae & Cancer Surgeries With Robotics


Know The Top 11 Benefits of Antenatal Exercises


FAQs
Can prolapse be cured without surgery?
Many women with mild to moderate prolapse improve significantly with supervised pelvic floor physiotherapy, pessary management, vaginal oestrogen, and lifestyle modifications. Surgery is reserved for cases that do not respond or where symptoms are severe.
Can Kegel exercises reverse prolapse?
Pelvic floor exercises can improve symptoms of mild prolapse and prevent progression. They cannot fully reverse moderate-to-severe prolapse, but they remain an important part of management at every stage — including after surgery.
What is a pessary and is it safe long-term?
A pessary is a silicone support device inserted vaginally. It is safe for long-term use with regular follow-up for cleaning and checking. Many women use a pessary for years and never need surgery.
Does prolapse surgery require uterus removal?
Not always. Uterine-preserving surgeries are available for selected patients. Whether to remove or preserve the uterus depends on the type and severity of prolapse, the patient’s age, fertility wishes, and individual anatomy.
Can prolapse come back after surgery?
Recurrence is possible in 10–30% of cases depending on risk factors. Addressing constipation, weight, chronic cough, and doing post-operative pelvic floor rehabilitation significantly reduces this risk.
Can I have sex after prolapse surgery?
Yes — in most cases, sexual function improves after prolapse repair because the anatomical correction relieves the physical barrier and discomfort. Intercourse is generally recommended from 6 weeks after surgery, once cleared at follow-up. The exception is colpocleisis, which permanently closes the vaginal canal.
What is robotic sacrocolpopexy?
A minimally invasive surgery performed through the da Vinci Xi robotic system to repair vault prolapse. Mesh is placed abdominally (not vaginally) to support the vaginal vault. It has the highest long-term success rate of any prolapse repair and is the preferred option for recurrent or complex prolapse at Fortis Mohali.
Which doctor should I see for prolapse?
A urogynaecologist — a sub-specialist trained specifically in pelvic floor disorders including prolapse, urinary incontinence, and voiding dysfunction. Fortis Mohali has the first dedicated urogynaecology service in the Tricity region.

Keep track of your appointments, get updates & more!

