






Why TAVR Is a Game Changer for Elderly Patients with Heart Valve Disease
Getting older often means dealing with health challenges younger people rarely face. When your cardiologist diagnoses severe aortic stenosis and mentions valve replacement, the thought of open-heart surgery can feel terrifying. For elderly patients, the risks seem even more significant. This is where TAVR has genuinely transformed cardiac care, offering treatment that was unimaginable just decades ago.
Understanding the Problem in Older Adults
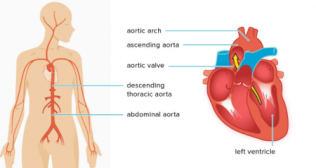
Aortic stenosis occurs when the valve between the heart’s main chamber and the aorta becomes stiff and narrow due to calcium buildup over time. As the valve tightens, blood flow drops, causing chest pain, breathlessness, and fatigue. Without treatment, severe cases can be life-threatening. In the past, surgical valve replacement was the only option, but many older patients were too fragile for open-heart surgery, leaving limited and often risky choices for care.
How TAVR Changed Everything
The TAVR procedure completely reimagined valve replacement by eliminating the need to open the chest and stop the heart. Instead, interventional cardiologists thread a catheter through a blood vessel, usually in the groin, and guide a compressed replacement valve to the heart. Once positioned correctly, the new valve expands and starts working immediately, pushing old calcified leaflets aside.
This approach transformed who could receive treatment. Patients in their eighties and nineties, those with significant lung disease, people with previous cardiac surgeries, and frail individuals who would never survive traditional surgery suddenly had options. The TAVR procedure made valve replacement accessible to populations previously without good choices.
The Recovery Difference
Perhaps the most dramatic advantage for elderly patients is the recovery timeline. After traditional TAVR surgery performed as open-heart surgery, patients typically spend a week hospitalized followed by months of restricted activity while breastbone heals. For an 85-year-old, this extended recovery can mean losing independence, needing temporary nursing home placement, and struggling to regain strength.
TAVR procedure recovery looks entirely different. Most patients spend just one or two nights hospitalized. The small groin incision heals within days. Within a week or two, many elderly patients report feeling better than they have in years as heart function improves and symptoms resolve. This rapid return helps maintain independence and quality of life in ways traditional surgery often cannot.
The difference is significant. Elderly patients undergoing TAVR frequently avoid complication cascades that can follow major surgery in this age group. Pneumonia, delirium, muscle wasting, and functional decline are all less common when recovery time is measured in days rather than months.
What Research Shows
Clinical trials have demonstrated impressive outcomes for elderly patients undergoing TAVR. Survival rates match or exceed traditional surgery in high-risk and intermediate-risk patients. More importantly, quality of life improvements appear more quickly after TAVR compared to surgical replacement.
Studies tracking patients over five years and beyond show valves placed via TAVR procedure demonstrate excellent durability. Early concerns these valves might not last as long as surgically placed ones have not materialized. Given life expectancy for someone in their eighties typically is less than projected valve lifespan, durability concerns become less relevant.
Complication rates favor TAVR in several important ways for elderly patients. Major bleeding occurs less frequently since there is no large chest incision. Atrial fibrillation happens less often with TAVR. Stroke risk exists with both approaches, though rates are generally low and continue improving as techniques evolve.
Important Considerations
TAVR is not perfect for everyone. The procedure requires adequate vascular access, meaning blood vessels in your groin or chest need to be large and healthy enough to accommodate the catheter. Severe peripheral artery disease can make access challenging or impossible. Anatomy matters too, as aortic root and valve shape need to accommodate the replacement valve properly.
Some patients need permanent pacemakers after TAVR because the procedure can affect the heart's electrical system. This happens in roughly 10 to 20 percent of cases depending on valve type used. For elderly patients, getting a pacemaker is a minor inconvenience compared to avoiding open-heart surgery.
Making the Decision
For older adults with severe aortic stenosis, the discussion with your cardiologist should center on overall health, life expectancy, and personal goals. Age alone doesn’t decide suitability. An active 88-year-old may do well with TAVR, while someone younger with serious illness may opt for comfort care instead. Most hospitals use a heart team approach, where cardiologists and surgeons review each case together to recommend the safest, most appropriate option.
Finding Experienced Care
TAVR surgery success depends heavily on team experience and expertise. High-volume centers develop protocols and skills translating into better outcomes and smoother recoveries. Elderly patients benefit particularly from centers understanding unique older adult needs, including medication management, cognitive status attention, and early mobilization.
The hospital in Delhi has extensive experience with structural heart procedures including TAVR, with outcomes reflecting their volume and expertise in treating complex cardiac conditions in older populations.
TAVR represents one of the most significant cardiovascular medicine advances for older adults. By making valve replacement accessible and tolerable for patients previously without good options, it has extended both length and quality of life for countless elderly individuals.
Categories
Clear allRelated Blogs
View all







FAQs

Keep track of your appointments, get updates & more!

