






Partial Nephrectomy for Kidney Tumours: When the Retroperitoneal Approach Makes a Difference
By Dr Dharmender Aggarwal Senior Consultant, Uro-Oncology & Robotic Surgery | Fortis Hospital, Mohali MCh Urology (PGIMER) | Fellowship in Robotic Surgery & Uro-Oncology (Royal College of Surgeons, England) ERUS Certified (Belgium) | ORSI Certified | 850+ Robotic Cancer Surgeries | Official Intuitive Proctor/Trainer
Removing the Tumour, Keeping the Kidney
“A kidney tumour diagnosis is frightening. But the conversation with patients has changed fundamentally in the last decade. For most small to medium kidney tumours, we no longer need to remove the entire kidney. Partial nephrectomy — removing only the tumour while preserving healthy kidney tissue — is now the standard of care. And for selected patients, we can do this through a route that does not enter the abdominal cavity at all: the retroperitoneal approach. This is a specialised technique that requires specific training and experience, but in the right hands and for the right tumour, it offers significant advantages in recovery, pain, and bowel function.”
If you have been diagnosed with a kidney tumour and are exploring your surgical options, this article explains what partial nephrectomy is, why preserving kidney tissue matters, how the retroperitoneal approach differs from the standard route, and when it is the right choice.
What Is a Partial Nephrectomy?
Partial nephrectomy means removing only the tumour-bearing portion of the kidney while preserving as much healthy tissue as possible. This is also called nephron-sparing surgery — because every unit of kidney function you keep matters, especially over a lifetime.
Both AUA (American Urological Association) and EAU (European Association of Urology) guidelines recommend partial nephrectomy as the preferred approach for most kidney tumours up to 7 cm (T1 stage), because it provides equivalent cancer control to radical nephrectomy (removing the entire kidney) while preserving renal function. This is particularly important for patients who have diabetes, hypertension, baseline kidney disease, a solitary kidney, or bilateral tumours — all of which are common in our North Indian patient population.
Two Routes to the Kidney: Transperitoneal vs Retroperitoneal
When performing a partial nephrectomy — whether robotic or laparoscopic — the surgeon must choose how to reach the kidney. There are two fundamentally different routes. But here is a fact that many patients find surprising: the kidney is itself a retroperitoneal organ — it naturally sits behind the peritoneal cavity, not inside it. Accessing it from the back, therefore, is anatomically the most direct route. It is the front approach that requires going through other structures to reach the kidney, not the other way around.
The transperitoneal approach goes through the front of the abdomen. The surgeon enters the peritoneal cavity, moves the bowels aside, and accesses the kidney from the front. This is the more commonly used route because it provides a larger working space and most urologists are trained in it first. But it involves handling the bowels, which can slow recovery and cause temporary bowel dysfunction (ileus).
The retroperitoneal approach reaches the kidney from behind, through the flank, without ever entering the abdominal cavity. Because the peritoneal cavity is never breached, the bowels are never touched — eliminating bowel handling entirely and with it, all bowel-related complications. The surgeon works in the retroperitoneal space — the anatomical compartment behind the peritoneum where the kidney naturally sits. This provides direct access to the kidney and its blood vessels, reducing console time because the surgeon reaches the target without first mobilising other organs. However, the working space is significantly smaller and the anatomy looks very different from the transperitoneal view. It requires specific training, a different learning curve, and substantial experience to perform safely.

What Are the Advantages of the Retroperitoneal Approach?
For the right patient and the right tumour, the retroperitoneal approach offers measurable clinical advantages. Because the kidney is a retroperitoneal organ, accessing it from behind is anatomically the most logical route — and the clinical benefits reflect this:
- Zero bowel handling — because the peritoneal cavity is never entered, there is no paralytic ileus (bowel paralysis). Patients are allowed oral intake within 6 hours of surgery — a dramatic difference from the transperitoneal route where bowel function may take 2–3 days to resume.
- Less post-operative pain — the abdominal wall muscles are not traversed, resulting in significantly less discomfort
- Shorter hospital stay — many patients are discharged within 24–48 hours, compared to 3–5 days with the transperitoneal route
- Direct access to the renal hilum — the kidney’s blood vessels (artery and vein) are accessed first, giving the surgeon early vascular control before the tumour is even visualised
- Ideal for patients with previous abdominal surgery — because the retroperitoneal space is untouched by prior operations, this approach completely avoids intra-abdominal adhesions that would make a transperitoneal approach significantly harder and riskier
- Better cosmetic outcome — small flank incisions that are naturally hidden by clothing
- No entry into peritoneal cavity — significantly reduces the chance of injury to surrounding intra-abdominal structures including bowel, spleen, and liver
- Oncologically equivalent — cancer control outcomes (negative margins, recurrence rates) are similar to transperitoneal robotic partial nephrectomy in published comparative data
Comparative studies published in peer-reviewed journals have demonstrated similar oncological and surgical outcomes between retroperitoneal and transperitoneal robotic partial nephrectomy, with some pooled analyses showing shorter operative time, lower blood loss, and shorter hospital stay in selected retroperitoneal cohorts.
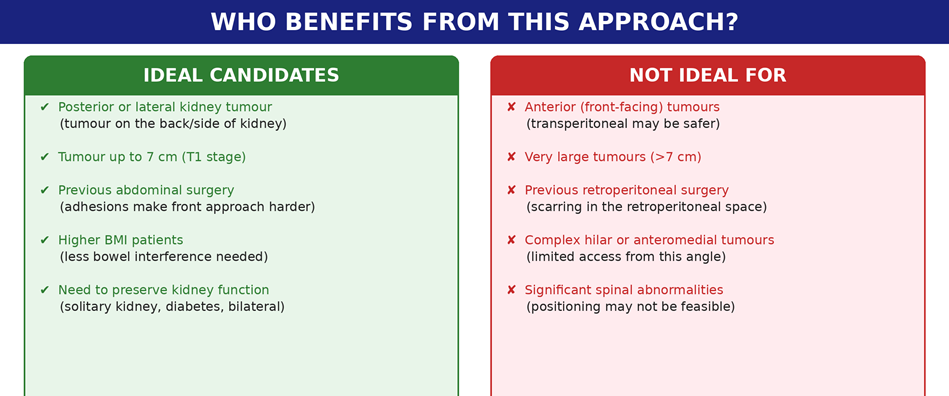
Who Benefits — and Who Does Not?
The retroperitoneal approach is not for every kidney tumour. It is a case-selection decision, and choosing the wrong route for a given tumour can make the surgery harder, not easier. The right approach depends on where the tumour is, not on which technique sounds more advanced.
Why This Approach Requires Specialised Expertise
The retroperitoneal space is anatomically confined. The surgeon works in a smaller cavity with different landmarks than the familiar transperitoneal view. All ports must be placed in a narrow space — unlike the transperitoneal approach where the entire abdominal wall is available for port positioning. The retroperitoneal space itself does not exist as a natural cavity — it must be created meticulously by the surgeon in the correct tissue plane to reach the kidney without breaching the peritoneal fold or injuring surrounding structures. This step alone requires significant experience and anatomical precision. CO₂ insufflation is then used to maintain the working space. The orientation of the kidney, vessels, and ureter is reversed compared to what most urologists see in their standard training. There are very few centres across the country performing this complex surgery routinely.
This is why retroperitoneal robotic partial nephrectomy is offered in select high-expertise robotic urology programmes rather than as a routine procedure. It is not about having the robot — many centres have robotic platforms. It is about having surgeons who are specifically trained, certified, and experienced in operating through this route.
At Fortis Mohali, our uro-oncology and robotic surgery programme is supported by dual Da Vinci Xi systems, a dedicated robotic urology team, and surgeon expertise in both retroperitoneal and transperitoneal approaches — so the route is chosen based on what is best for the individual tumour, not on what the surgeon is most comfortable with. Having completed over 850 robotic cancer surgeries, including a significant proportion of retroperitoneal partial nephrectomies, the programme has the volume and experience to offer this specialised technique routinely and safely.
From the Practice: A Case That Shows the Difference
“A 54-year-old man from Ludhiana was referred to us with a 4.5 cm tumour on the posterior surface of his right kidney. He had previously undergone open surgery for a perforated duodenal ulcer, leaving significant intra-abdominal adhesions. Two centres had recommended radical nephrectomy (complete kidney removal) because of the adhesions and tumour location. We assessed the case and determined that a retroperitoneal robotic partial nephrectomy was feasible — the posterior location was ideal for this route, and the retroperitoneal space was unaffected by his previous abdominal surgery. The procedure took approximately 2.5 hours. He was eating the same evening, walking the next morning, and discharged at 36 hours with normal kidney function. Pathology confirmed clear margins. His kidney was preserved.”
Your Kidney-Sparing Surgery Journey
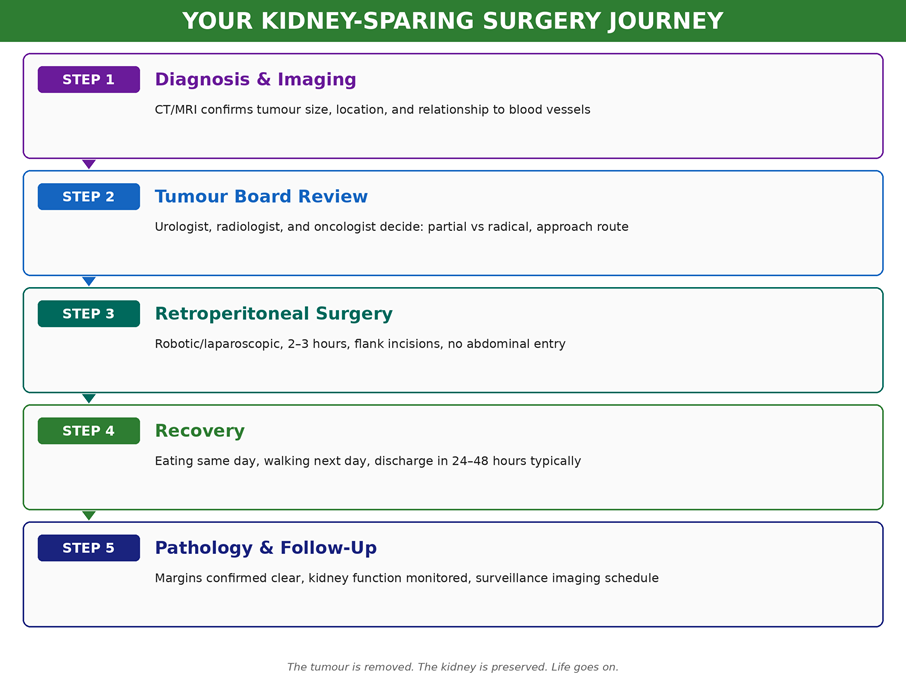
If you have been diagnosed with a kidney tumour and want to understand whether kidney-sparing surgery is an option — and whether the retroperitoneal approach is right for your specific tumour — schedule a consultation with Dr Dharmender Aggarwal at Fortis Hospital Mohali. Bring your CT scan and any previous reports for a comprehensive assessment. We welcome second opinions and referrals from across North India.
About the Author
Dr Dharmender Aggarwal is a Senior Consultant in Uro-Oncology and Robotic Surgery at Fortis Hospital, Mohali. He completed his MBBS from Madurai Medical College, MS in General Surgery from Maulana Azad Medical College, New Delhi, and MCh in Urology from PGIMER, Chandigarh. He trained in robotic surgery for urological cancers for over two years in London and holds a Fellowship in Robotic Surgery and Uro-Oncology from the Royal College of Surgeons, England (St George’s NHS Hospital). He is certified by the European Robotic Urology Section (ERUS) and ORSI Academy, Belgium. Dr Aggarwal has performed over 850 robotic cancer surgeries and 3,500+ urological procedures, and serves as an official proctor/trainer for Intuitive Surgical, having helped establish robotic programmes at multiple centres across India. His sub-specialty focus is robotic surgery for cancers of the kidney, bladder, prostate, and upper urinary tract, with particular expertise in retroperitoneal approaches to kidney tumour surgery.
Categories
Clear allMeet the doctor

- Urology | Uro-Oncology | Urology
-
 9 Years
9 Years
-
 1050
1050
Related Blogs
View all


Adult Circumcision: Debunking Facts and Myths | Fortis Health Connect Blogs

Is Beer Good for Kidney Stones ? - Myths Vs Facts | Fortis Healthcare



FAQs
Is partial nephrectomy better than removing the whole kidney?
For most tumours up to 7 cm, yes. Both AUA and EAU guidelines recommend partial nephrectomy because it provides equivalent cancer control while preserving kidney function. Removing the entire kidney is reserved for very large tumours, tumours that cannot be safely separated from critical structures, or situations where partial nephrectomy is technically not feasible.
Is the retroperitoneal approach suitable for every kidney tumour?
Although, it is best suited for posterior and lateral tumours, many anterior tumours and large tumours also may be operated with this approach in experienced hands. On the other hand, complex hilar tumours, and patients with prior retroperitoneal surgery may be better served by the transperitoneal route. The choice is made individually for each patient based on CT imaging and clinical assessment.

Keep track of your appointments, get updates & more!

