






My NIPT Came Back High-Risk - What Happens Now?
By Dr Ravneet Kaur Consultant, Medical Genetics & Genomic Medicine | Fortis Hospital, Mohali DM Medical Genetics (AIIMS, New Delhi) | Fortis Institute of Genomic Medicine
⚠️ KEY TAKEAWAY: A high-risk NIPT result is NOT a diagnosis. NIPT is a screening test that estimates probability. False positives are common — especially for rarer conditions and in younger women. No irreversible pregnancy decision should ever be made based on NIPT alone. Confirmatory diagnostic testing (CVS or amniocentesis) is the only way to know for certain.
First, Take a Breath
Receiving a high-risk NIPT result can feel like the ground has shifted beneath you. The anxiety is immediate and overwhelming. But before that anxiety becomes a decision, you need to understand what this result actually means — and what it does not mean. In my years of genetic counselling at the Fortis Institute of Genomic Medicine, I have seen hundreds of high-risk NIPT results. Many — more than most families expect — turn out to be false positives after confirmatory testing. A high-risk result opens a conversation. It does not close one.
If you are reading this because your NIPT came back high-risk, this guide is written for you. It will walk you through exactly what the result means, why false positives happen, what confirmatory tests are available, and how to make informed decisions based on facts — not fear.
What NIPT Actually Tests — and What It Cannot Tell You
NIPT (Non-Invasive Prenatal Testing) analyses fragments of cell-free DNA circulating in the mother’s blood during pregnancy. Critically, most of this DNA comes from the placenta, not directly from the baby. The test screens for chromosomal abnormalities by measuring whether there is more or less DNA from specific chromosomes than expected.
NIPT screens for trisomy 21 (Down syndrome), trisomy 18 (Edwards syndrome), trisomy 13 (Patau syndrome), and in some panels, sex chromosome abnormalities and select microdeletions. It has a high detection rate for trisomy 21 — approximately 99% sensitivity — which means it catches nearly all true cases. But sensitivity is not the same as certainty.
A high-risk NIPT means there is an increased probability that the baby may have a chromosomal condition. It does not mean the baby has it. The difference between probability and diagnosis is the most important thing to understand right now.
Why False Positives Happen — and How Common They Are
This is the section that most families need to read carefully. A false positive means the NIPT flagged a high-risk result, but the baby is chromosomally normal. False positives are more common than most people realise — and they occur for real biological reasons, not because the test is “bad.”
Confined Placental Mosaicism (CPM)
Because NIPT analyses placental DNA, it reflects the placenta’s chromosomal makeup — which can sometimes differ from the baby’s. In confined placental mosaicism, the placenta carries an abnormal chromosomal line that the baby does not. The NIPT reads the placental abnormality and reports a high-risk result, but the baby is genetically normal. This is the single most common cause of false positive NIPT results.
Vanishing Twin
In early pregnancy, a twin embryo may stop developing and be reabsorbed. The cell-free DNA from this non-viable twin can persist in the mother’s bloodstream and be detected by NIPT, producing a high-risk result that does not reflect the surviving baby.
Maternal Factors
Rarely, the mother herself may carry chromosomal variations, benign copy number changes, or undiagnosed conditions that contribute to an altered DNA signal. These have nothing to do with the baby’s health.
The Numbers You Need to Know
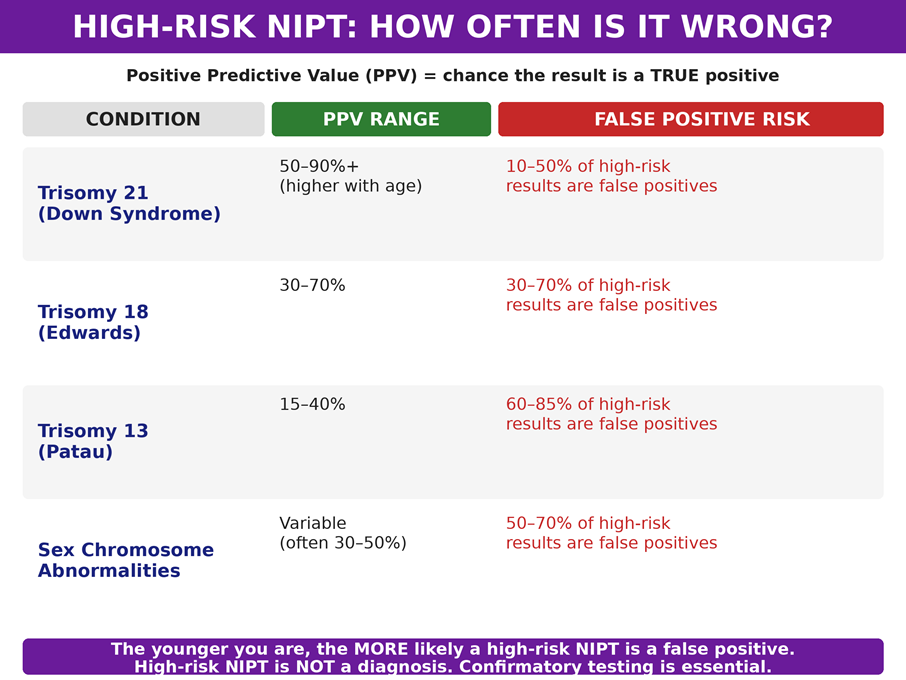
The critical insight: for rarer conditions like trisomy 13 and sex chromosome abnormalities, the majority of high-risk NIPT results are false positives. Even for trisomy 21, where NIPT is most accurate, 10–50% of high-risk results in younger women turn out to be false positives after confirmatory testing. This is why diagnostic testing is essential.
“In my practice, I have counselled hundreds of families after high-risk NIPT results. The most important message I share is this: do not let a screening result make a decision that only a diagnostic test should make. I have seen too many families in distress because they interpreted ‘high-risk’ as ‘confirmed.’ In many of those cases, the confirmatory test came back completely normal.” — Dr Ravneet Kaur, DM Medical Genetics (AIIMS, New Delhi)
Your Roadmap: What Happens After a High-Risk NIPT
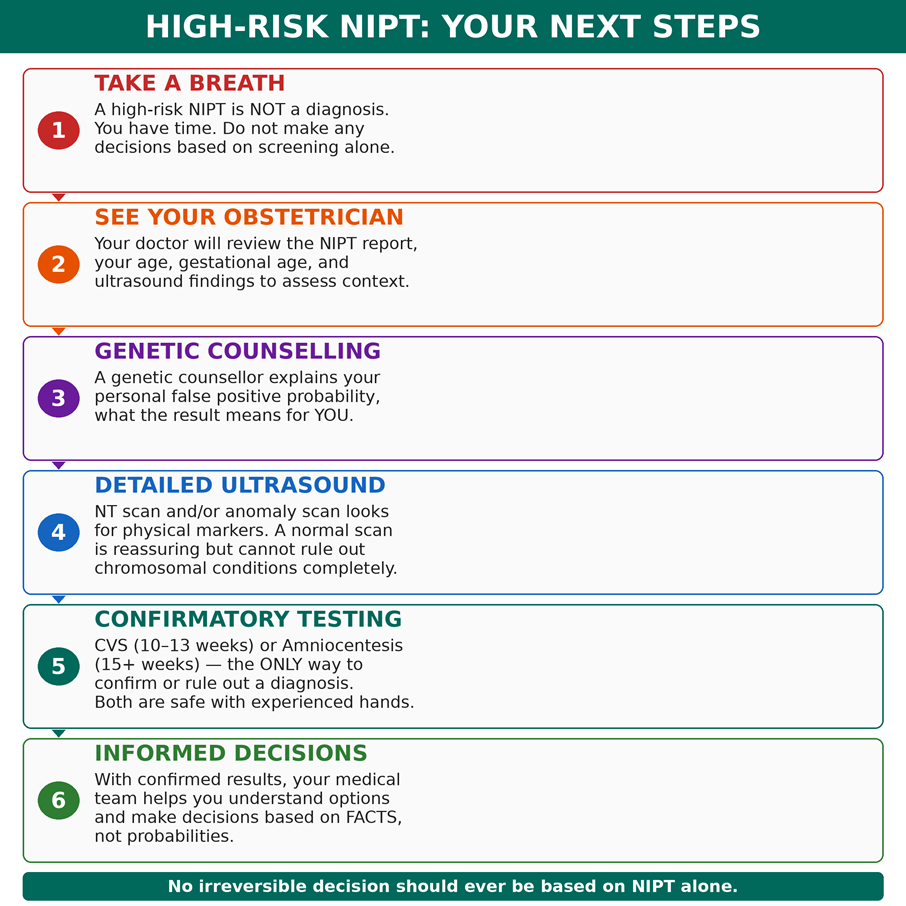
Step 1: Genetic Counselling — Understanding Your Personal Risk
The first step after any high-risk NIPT is a genetic counselling session — ideally within the same week. The genetic counsellor or medical geneticist will review your NIPT report in the context of your age, gestational age, ultrasound findings, and the specific condition flagged. They will calculate your personal positive predictive value (PPV) — which may be very different from the general population PPV.
A 25-year-old with a high-risk NIPT for trisomy 21 has a much higher false positive probability than a 40-year-old with the same result, because the baseline prevalence of trisomy 21 is much lower in younger women. Your counsellor will help you understand what the result means for you specifically — not in general.
Step 2: Detailed Ultrasound — What It Can and Cannot Tell You
A detailed ultrasound — including nuchal translucency (NT) measurement in the first trimester, and a comprehensive anomaly scan in the second trimester — can look for physical markers associated with chromosomal conditions. A thickened NT, absent nasal bone, cardiac defects, and shortened long bones may increase concern. However, a completely normal ultrasound cannot rule out a chromosomal condition. Many babies with trisomy 21 have no ultrasound abnormalities.
The ultrasound adds context. It does not replace diagnostic testing.
Step 3: Confirmatory Diagnostic Testing — The Only Way to Know
No major professional organisation — not ACOG, not SMFM, not ISUOG — recommends making irreversible pregnancy decisions based solely on NIPT. Confirmatory diagnostic testing is the universally recommended next step.
Chorionic Villus Sampling (CVS) — 10–13 Weeks
A small sample of placental tissue is collected under ultrasound guidance. Results are available within 7–10 days (preliminary FISH results in 2–3 days). CVS offers the advantage of an earlier answer, allowing families more time for decision-making. Limitation: Because CVS samples the placenta (not the baby directly), in rare cases it may reflect confined placental mosaicism rather than true fetal chromosome status. Procedure-related miscarriage risk is very low — approximately 1 in 500 when performed by experienced hands.
Amniocentesis — 15 Weeks Onwards
A small sample of amniotic fluid containing the baby’s own shed cells is collected under ultrasound guidance. Amniocentesis is often considered the definitive gold standard because it tests the baby’s actual cells, not the placenta. Results take 10–14 days for full karyotype (FISH in 2–3 days). It can also screen for neural tube defects. Procedure-related miscarriage risk is very low — approximately 1 in 900.
Both CVS and amniocentesis are safe when performed by experienced fetal medicine specialists. The choice between them depends primarily on gestational age and your preference for earlier versus more definitive results. Your geneticist and obstetrician will guide this decision based on your specific situation.
What If Confirmatory Testing Confirms the Diagnosis?
If diagnostic testing confirms that the baby does have a chromosomal condition, your medical team — including the geneticist, obstetrician, and, where appropriate, paediatric specialists — will provide comprehensive counselling about the specific condition, its clinical spectrum, expected outcomes, and available options. Conditions like trisomy 21 have a wide clinical spectrum, and families benefit from hearing about the range of outcomes, support services, and lived experiences before making any decisions.
The goal of this entire process is to ensure that any decision you make is based on confirmed facts, complete information, and adequate time — not on a screening probability read at 2 AM on a phone screen.
If your NIPT has come back high-risk, the next step is genetic counselling — not Google. Schedule a consultation with Dr Ravneet Kaur at the Fortis Institute of Genomic Medicine, Fortis Hospital Mohali. With a detailed review of your report, your age, your ultrasound, and your personal risk profile, we will help you understand what this result means for you specifically and guide you through confirmatory testing if needed. You are not alone in this, and you have time to make informed decisions.
About the Author
Dr Ravneet Kaur is a Consultant in Medical Genetics and Genomic Medicine at Fortis Hospital, Mohali. She completed her DM in Medical Genetics from AIIMS, New Delhi — India’s premier institution for clinical genetics training. Dr Kaur leads the Fortis Institute of Genomic Medicine, providing genetic counselling, prenatal diagnosis, cancer genomics, and precision medicine support. Her clinical focus includes prenatal genetic screening (NIPT, carrier screening), confirmatory diagnostic testing coordination, and genetic counselling for families navigating complex results. She works closely with the Department of Obstetrics and Fetal Medicine to ensure that every high-risk prenatal result is followed by expert-guided, evidence-based next steps. References: ACOG Practice Bulletin No. 226 (2020), SMFM Consult Series #36, ISUOG Practice Guidelines, Cochrane Review on NIPT Accuracy.
Categories
Clear allRelated Blogs
View all
Unraveling the power of genes: A lot more than how you look

Breakthrough Discoveries in Genetic Research: Unlocking the Secrets of DNA and Heredity

CHIP Mutations in Hematology: The Silent Forecasters of Risk

Genomics in Hematology: Redefining Diagnosis and Therapy at Fortis Institute of Genomic Me...
Decoding the Mystery of Rare Diseases: A Family’s Guide to Medical Genetics

Why NIPT Matters in Your Pregnancy The Simple Blood Test That Gives You Answers from 10 We...


FAQs
Can a high-risk NIPT be wrong?
Yes. False positives occur for biological reasons including confined placental mosaicism, vanishing twin, and maternal factors. Depending on the condition and the mother’s age, anywhere from 10% to 85% of high-risk NIPT results are false positives. Confirmatory diagnostic testing is the only way to determine whether the result reflects the baby’s actual chromosomes.
Should I repeat the NIPT instead of doing an invasive test?
Generally, no. A repeat NIPT will likely return the same result because the underlying biology (e.g., placental mosaicism) has not changed. Diagnostic testing (CVS or amniocentesis) provides a definitive answer that a repeat screening test cannot.
Is CVS safer than amniocentesis?
Both are considered very safe when performed by experienced specialists. The procedure-related miscarriage risk is approximately 1 in 500 for CVS and 1 in 900 for amniocentesis. The choice depends on gestational age, the specific situation, and your preference for timing of results.
Should I make a pregnancy decision based on NIPT alone?
No. Every major professional guideline — ACOG, SMFM, ISUOG — recommends confirmatory diagnostic testing before any irreversible decision. NIPT is a screening tool with known false positive rates. Decisions should be based on confirmed diagnoses, not probabilities.
Does a false positive NIPT mean something is wrong with me?
No. A false positive usually reflects the placenta, not you or the baby. Confined placental mosaicism is a normal biological variation. It does not indicate that you have a health problem or that future pregnancies are at increased risk.
How long do confirmatory test results take?
Preliminary FISH results are usually available in 2–3 days. A full karyotype or microarray takes 10–14 days. Your geneticist will discuss the timeline and what each level of result tells you.

Keep track of your appointments, get updates & more!

